

Liver-First Approach for Synchronous Colorectal Metastases: Analysis of 7360 Patients from the LiverMetSurvey Registry
- PMID: 34212254
- PMCID: PMC8590998
- DOI: 10.1245/s10434-021-10220-w
Liver-First Approach for Synchronous Colorectal Metastases: Analysis of 7360 Patients from the LiverMetSurvey Registry
Abstract
Background: The liver-first approach in patients with synchronous colorectal liver metastases (CRLM) has gained wide consensus but its role is still to be clarified. We aimed to elucidate the outcome of the liver-first approach and to identify patients who benefit at most from this approach.
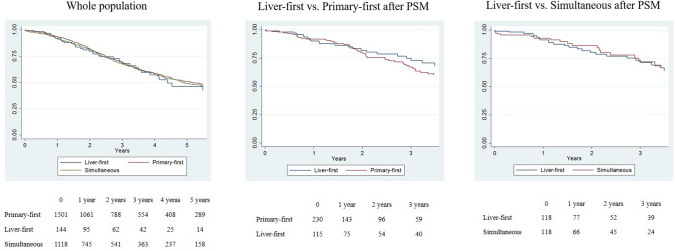
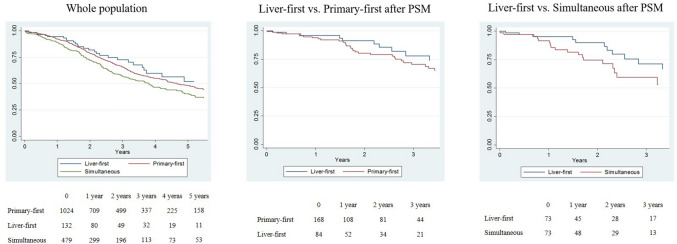
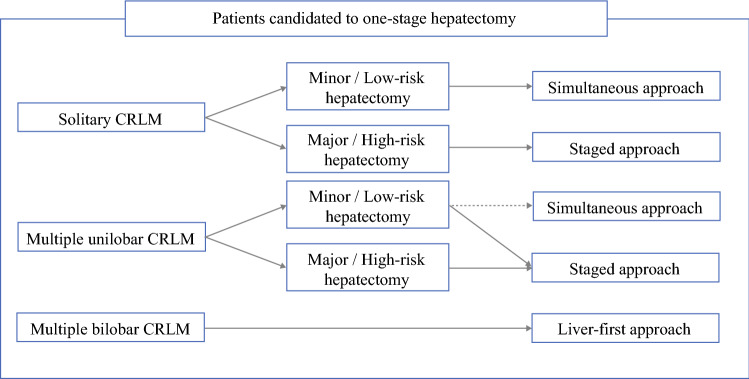
Methods: Patients with synchronous CRLM included in the LiverMetSurvey registry between 2000 and 2017 were considered. Three strategies were analyzed, i.e. liver-first approach, colorectal resection followed by liver resection (primary-first), and simultaneous resection, and three groups of patients were analyzed, i.e. solitary metastasis, multiple unilobar CRLM, and multiple bilobar CRLM. In each group, patients from the three strategy groups were matched by propensity score analysis.
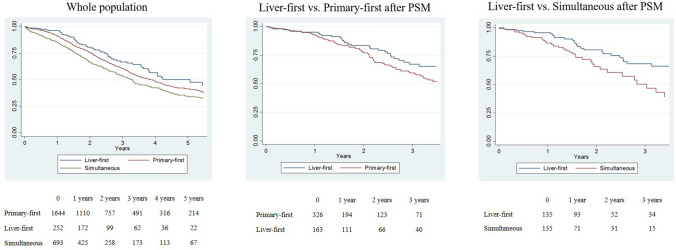
Results: Overall, 7360 patients were analyzed: 4415 primary-first, 552 liver-first, and 2393 simultaneous resections. Compared with the other groups, the liver-first group had more rectal tumors (58.0% vs. 31.2%) and higher hepatic tumor burden (more than three CRLMs: 34.8% vs. 24.0%; size > 50 mm: 35.6% vs. 22.8%; p < 0.001). In patients with solitary and multiple unilobar CRLM, survival was similar regardless of treatment strategy, whereas in patients with multiple bilobar metastases, the liver-first approach was an independent positive prognostic factor, both in unmatched patients (3-year survival 65.9% vs. primary-first 60.4%: hazard ratio [HR] 1.321, p = 0.031; vs. simultaneous resections 54.4%: HR 1.624, p < 0.001) and after propensity score matching (vs. primary-first: HR 1.667, p = 0.017; vs. simultaneous resections: HR 2.278, p = 0.003).
Conclusion: In patients with synchronous CRLM, the surgical strategy should be decided according to the hepatic tumor burden. In the presence of multiple bilobar CRLM, the liver-first approach is associated with longer survival than the alternative approaches and should be evaluated as standard.
© 2021. The Author(s).
Figures
Comment in
-
ASO Author Reflections: The Liver-First Approach: A New Standard for Patients with Multiple Bilobar Colorectal Metastases?Ann Surg Oncol. 2021 Dec;28(13):8209-8210. doi: 10.1245/s10434-021-10272-y. Epub 2021 Jul 26. Ann Surg Oncol. 2021. PMID: 34312801 No abstract available.
References
-
- Ferlay J, Colombet M, Soerjomataram I, et al. Cancer incidence and mortality patterns in Europe: estimates for 40 countries and 25 major cancers in 2018. Eur J Cancer. 2018;103:356–387. - PubMed
-
- The International Agency for Research on Cancer (IARC): New Global Cancer Data: GLOBOCAN 2018. https://www.uicc.org/new-global-cancer-data-globocan-2018#
-
- Viganò L, Ferrero A, Lo Tesoriere R, et al. Liver surgery for colorectal metastases: results after 10 years of follow-up. Long-term survivors, late recurrences, and prognostic role of morbidity. Ann Surg Oncol. 2008;15:2458–2464. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
