

BOLD asynchrony elucidates tumor burden in IDH-mutated gliomas
- PMID: 34214170
- PMCID: PMC8730764
- DOI: 10.1093/neuonc/noab154
BOLD asynchrony elucidates tumor burden in IDH-mutated gliomas
Abstract
Background: Gliomas comprise the most common type of primary brain tumor, are highly invasive, and often fatal. IDH-mutated gliomas are particularly challenging to image and there is currently no clinically accepted method for identifying the extent of tumor burden in these neoplasms. This uncertainty poses a challenge to clinicians who must balance the need to treat the tumor while sparing healthy brain from iatrogenic damage. The purpose of this study was to investigate the feasibility of using resting-state blood oxygen level-dependent (BOLD) functional magnetic resonance imaging (fMRI) to detect glioma-related asynchrony in vascular dynamics for distinguishing tumor from healthy brain.
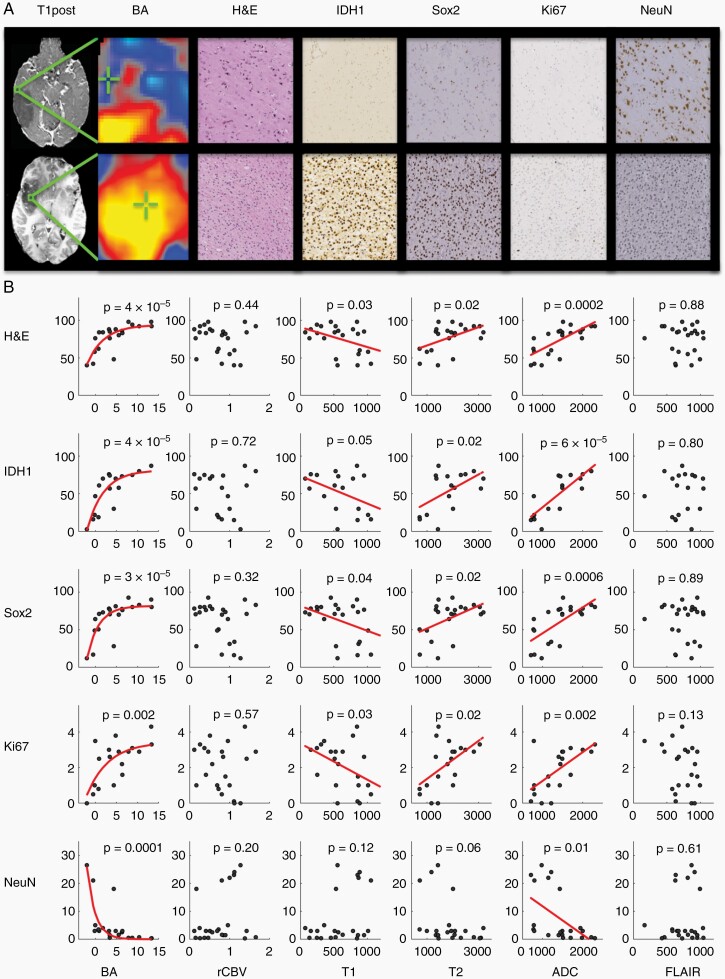
Methods: Twenty-four stereotactically localized biopsies were obtained during open surgical resection from ten treatment-naïve patients with IDH-mutated gliomas who received standard-of-care preoperative imaging as well as echo-planar resting-state BOLD fMRI. Signal intensity for BOLD asynchrony and standard-of-care imaging was compared to cell counts of total cellularity (H&E), tumor density (IDH1 & Sox2), cellular proliferation (Ki67), and neuronal density (NeuN), for each corresponding sample.
Results: BOLD asynchrony was directly related to total cellularity (H&E, P = 4 × 10-5), tumor density (IDH1, P = 4 × 10-5; Sox2, P = 3 × 10-5), cellular proliferation (Ki67, P = .002), and inversely related to neuronal density (NeuN, P = 1 × 10-4).
Conclusions: Asynchrony in vascular dynamics, as measured by resting-state BOLD fMRI, correlates with tumor burden and provides a radiographic delineation of tumor boundaries in IDH-mutated gliomas.
Keywords: BOLD asynchrony; IDH-mutated glioma; infiltration; resting-state fMRI; tumor burden.
© The Author(s) 2021. Published by Oxford University Press on behalf of the Society for Neuro-Oncology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
Comment in
-
BOLD asynchrony: An imaging biomarker of tumor burden in IDH-mutated gliomas.Neuro Oncol. 2022 Jan 5;24(1):88-89. doi: 10.1093/neuonc/noab248. Neuro Oncol. 2022. PMID: 34695182 Free PMC article. No abstract available.
References
-
- Oszvald A, Güresir E, Setzer M, et al. . Glioblastoma therapy in the elderly and the importance of the extent of resection regardless of age. J Neurosurg. 2012;116(2):357–364. - PubMed
-
- Sanai N, Polley MY, McDermott MW, Parsa AT, Berger MS. An extent of resection threshold for newly diagnosed glioblastomas. J Neurosurg. 2011;115(1):3–8. - PubMed
-
- Waldman AD, Jackson A, Price SJ, et al. . Quantitative imaging biomarkers in neuro-oncology. Nat Rev Clin Oncol. 2009;6(8):445–454. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
