

Immunogenicity of SARS-CoV-2 messenger RNA vaccines in patients with cancer
- PMID: 34214473
- PMCID: PMC8218532
- DOI: 10.1016/j.ccell.2021.06.009
Immunogenicity of SARS-CoV-2 messenger RNA vaccines in patients with cancer
Abstract
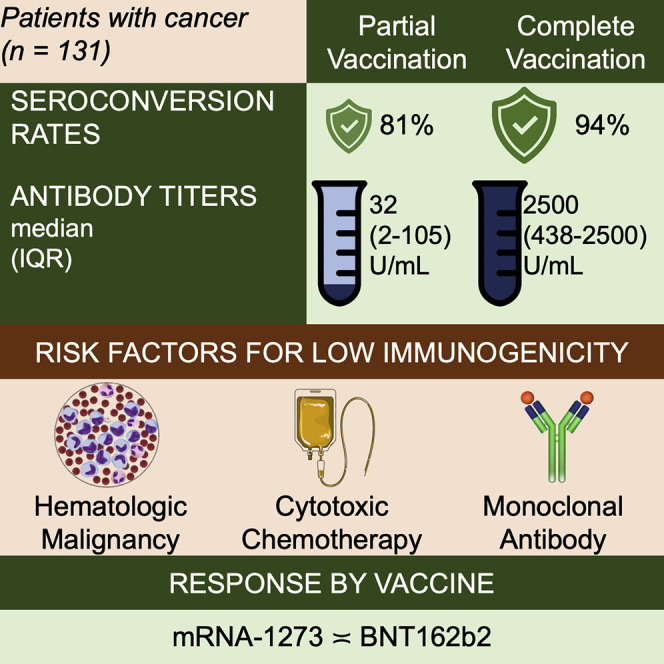
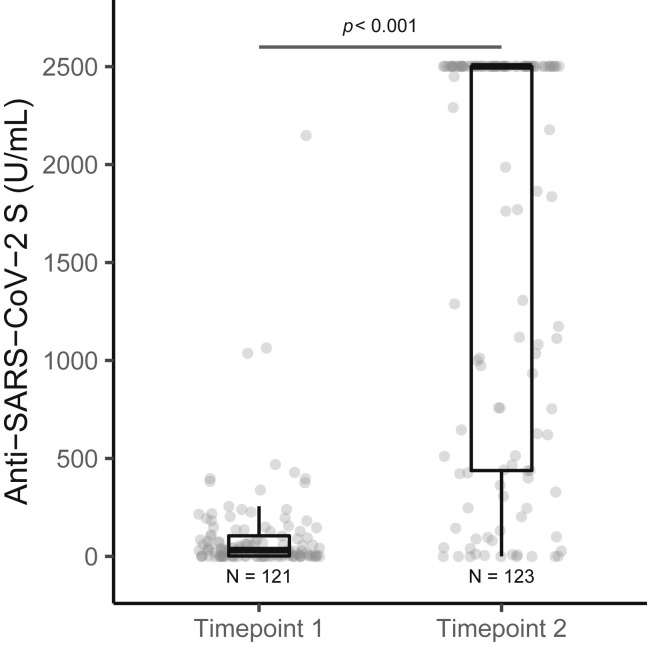
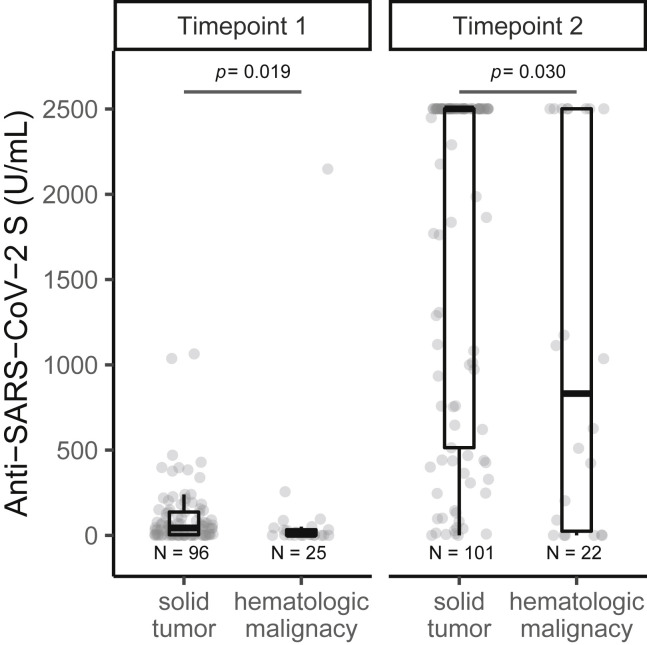
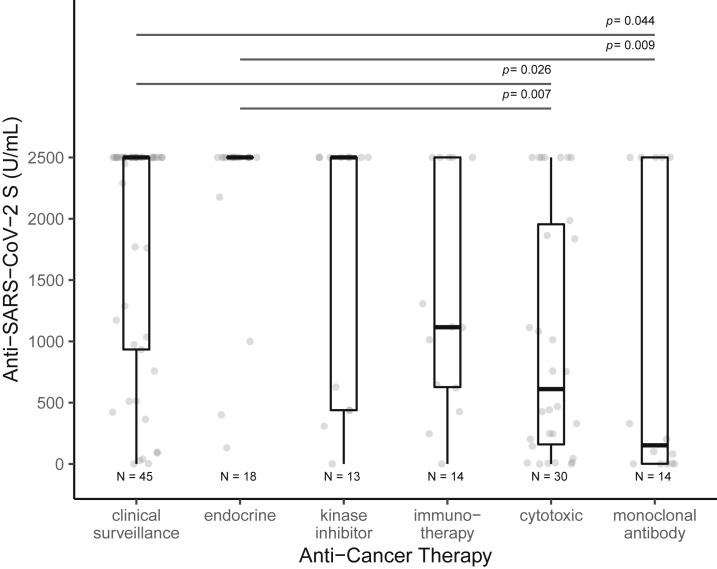
Patients with cancer experience a higher burden of SARS-CoV-2 infection, disease severity, complications, and mortality, than the general population. SARS-CoV-2 mRNA vaccines are highly effective in the general population; however, few data are available on their efficacy in patients with cancer. Using a prospective cohort, we assessed the seroconversion rates and anti-SARS-CoV-2 spike protein antibody titers following the first and second dose of BNT162b2 and mRNA-1273 SARS-CoV-2 vaccines in patients with cancer in US and Europe from January to April 2021. Among 131 patients, most (94%) achieved seroconversion after receipt of two vaccine doses. Seroconversion rates and antibody titers in patients with hematological malignancy were significantly lower than those with solid tumors. None of the patients with history of anti-CD-20 antibody in the 6 months before vaccination developed antibody response. Antibody titers were highest for clinical surveillance or endocrine therapy groups and lowest for cytotoxic chemotherapy or monoclonal antibody groups.
Keywords: COVID-19; anti-cancer treatment; antibody; immune response; malignancy; oncology; pandemic; seroconversion; tumor; vaccine.
Copyright © 2021 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests A.A. reported receiving personal fees for attending advisory from Bristol-Myers Squibb, AstraZeneca, Roche, Pfizer, Merck Sharp and Dohme, Astella, Eli Lilly, and Boehringer Ingelheim and receiving fees for speaking bureau for Eli Lilly, AstraZeneca, Merck Sharp and Dohme for work performed outside of this study. P.S. reported receiving a grant from the Biomedical Advanced Research and Development Authority outside of this work. I.L.-G. reported receiving personal fees for attending advisory from AstraZeneca. N.M. is a founder and minority shareholder of MaxiVAX SA, a private biotech company based in Geneva, Switzerland, working on personalized cancer immunotherapy and infectious disease vaccines, with no impact on the current manuscript. R.M. reported receiving research support from Celgene, Incyte, Abbvie, Samus, Genotech, Promedior, and CTI; and consulting fees from Novartis, Sierra Onc, LaJolla, and Pharma. D.S. reported receiving a grant from the Biomedical Advanced Research and Development Authority outside of this work. All other co-authors reported no competing interests.
Figures
Comment in
-
Immunogenicity of a heterologous COVID-19 vaccine after failed vaccination in a lymphoma patient.Cancer Cell. 2021 Aug 9;39(8):1037-1038. doi: 10.1016/j.ccell.2021.06.015. Epub 2021 Jun 26. Cancer Cell. 2021. PMID: 34242571 Free PMC article. No abstract available.
-
Highly variable SARS-CoV-2 spike antibody responses to two doses of COVID-19 RNA vaccination in patients with multiple myeloma.Cancer Cell. 2021 Aug 9;39(8):1028-1030. doi: 10.1016/j.ccell.2021.06.014. Epub 2021 Jun 29. Cancer Cell. 2021. PMID: 34242572 Free PMC article. No abstract available.
References
-
- Alvim R.G.F., Lima T.M., Rodrigues D.A.S., Marsili F.F., Bozza V.B.T., Higa L.M., Monteiro F.L., Abreu D.P.B., Leitão I.C., Carvalho R.S., et al. An affordable anti-SARS-COV-2 spike protein ELISA test for early detection of IgG seroconversion suited for large-scale surveillance studies in low-income countries. medRxiv. 2020 doi: 10.1101/2020.07.13.20152884. - DOI
-
- Barrière J., Chamorey E., Adjtoutah Z., Castelnau O., Mahamat A., Marco S., Petit E., Leysalle A., Raimondi V., Carles M. Impaired immunogenicity of BNT162b2 anti-SARS-CoV-2 vaccine in patients treated for solid tumors. Ann. Oncol. 2021;S0923-7534:01183–01184. doi: 10.1016/j.annonc.2021.04.019. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
