

Stillbirth as left truncation for early neonatal death in California, 1989-2015: a time-series study
- PMID: 34215208
- PMCID: PMC8252318
- DOI: 10.1186/s12884-021-03852-z
Stillbirth as left truncation for early neonatal death in California, 1989-2015: a time-series study
Abstract
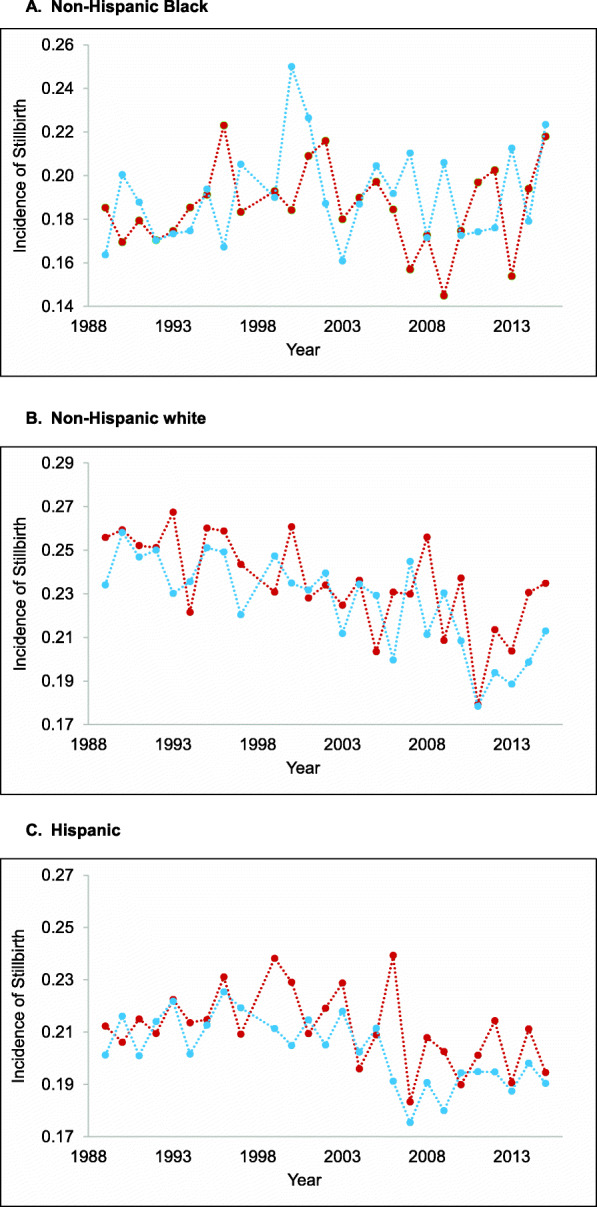
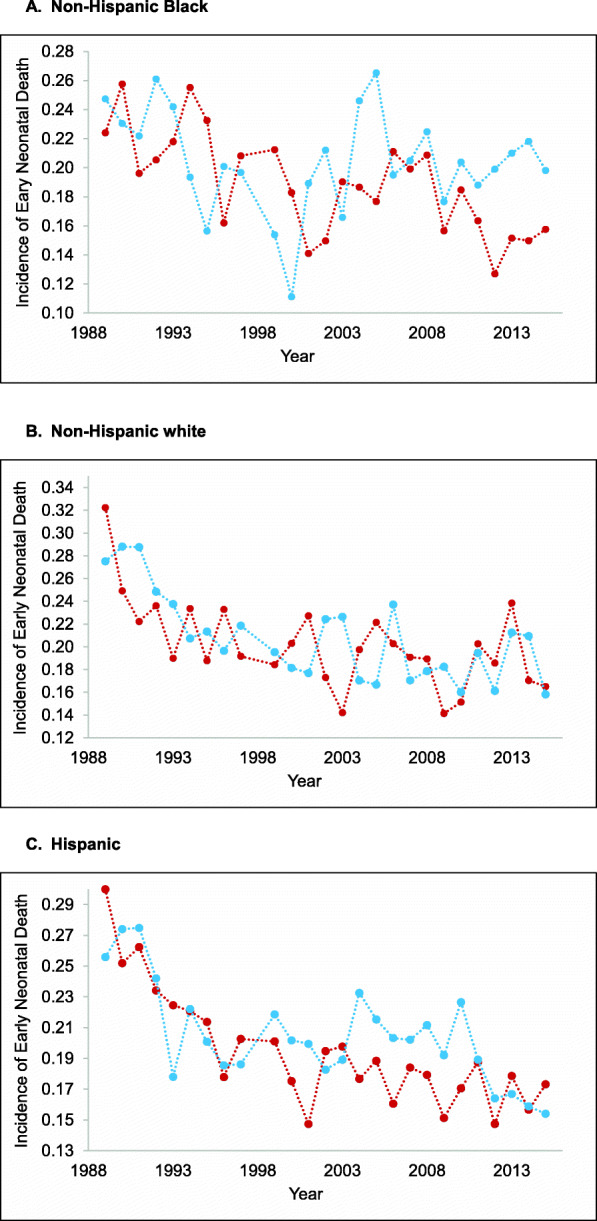
Background: Some scholars posit that attempts to avert stillbirth among extremely preterm gestations may result in a live birth but an early neonatal death. The literature, however, reports no empirical test of this potential form of left truncation. We examine whether annual cohorts delivered at extremely preterm gestational ages show an inverse correlation between their incidence of stillbirth and early neonatal death.
Methods: We retrieved live birth and infant death information from the California Linked Birth and Infant Death Cohort Files for years 1989 to 2015. We defined the extremely preterm period as delivery from 22 to < 28 weeks of gestation and early neonatal death as infant death at less than 7 days of life. We calculated proportions of stillbirth and early neonatal death separately by cohort year, race/ethnicity, and sex. Our correlational analysis controlled for well-documented declines in neonatal mortality over time.
Results: California reported 89,276 extremely preterm deliveries (live births and stillbirths) to Hispanic, non-Hispanic (NH) Black, and NH white mothers from 1989 to 2015. Findings indicate an inverse correlation between stillbirth and early neonatal death in the same cohort year (coefficient: -0.27, 95% CI of - 0.11; - 0.42). Results remain robust to alternative specifications and falsification tests.
Conclusions: Findings support the notion that cohorts with an elevated risk of stillbirth also show a reduced risk of early neonatal death among extremely preterm deliveries. Results add to the evidence base that selection in utero may influence the survival characteristics of live-born cohorts.
Keywords: Left truncation Bias; Live birth; Neonatal death; Stillbirth.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Stoll BJ, Hansen NI, Bell EF, Walsh MC, Carlo WA, Shankaran S, Laptook AR, Sánchez PJ, van Meurs K, Wyckoff M, Das A, Hale EC, Ball MB, Newman NS, Schibler K, Poindexter BB, Kennedy KA, Cotten CM, Watterberg KL, D'Angio CT, DeMauro S, Truog WE, Devaskar U, Higgins RD, Eunice Kennedy Shriver National Institute of Child Health and Human Development Neonatal Research Network Trends in care practices, morbidity, and mortality of extremely preterm neonates, 1993-2012. JAMA. 2015;314(10):1039–1051. doi: 10.1001/jama.2015.10244. - DOI - PMC - PubMed
-
- Stoll BJ, Hansen NI, Bell EF, Shankaran S, Laptook AR, Walsh MC, Hale EC, Newman NS, Schibler K, Carlo WA, Kennedy KA, Poindexter BB, Finer NN, Ehrenkranz RA, Duara S, Sanchez PJ, O'Shea TM, Goldberg RN, van Meurs KP, Faix RG, Phelps DL, Frantz ID, Watterberg KL, Saha S, Das A, Higgins RD, for the Eunice Kennedy Shriver National Institute of Child Health and Human Development Neonatal Research Network Neonatal outcomes of extremely preterm infants from the NICHD neonatal research network. Pediatrics. 2010;126(3):443–456. doi: 10.1542/peds.2009-2959. - DOI - PMC - PubMed
-
- Patel RM, Kandefer S, Walsh MC, Bell EF, Carlo WA, Laptook AR, Sánchez PJ, Shankaran S, van Meurs K, Ball MB, Hale EC, Newman NS, Das A, Higgins RD, Stoll BJ, Eunice Kennedy Shriver National Institute of Child Health and Human Development Neonatal Research Network Causes and timing of death in extremely premature infants from 2000 through 2011. N Engl J Med. 2015;372(4):331–340. doi: 10.1056/NEJMoa1403489. - DOI - PMC - PubMed
