

Imaging biomarkers for evaluating tumor response: RECIST and beyond
- PMID: 34215324
- PMCID: PMC8252278
- DOI: 10.1186/s40364-021-00306-8
Imaging biomarkers for evaluating tumor response: RECIST and beyond
Abstract
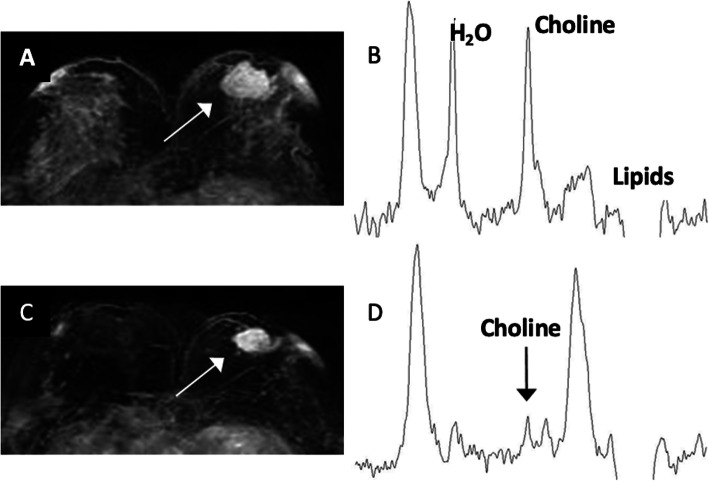
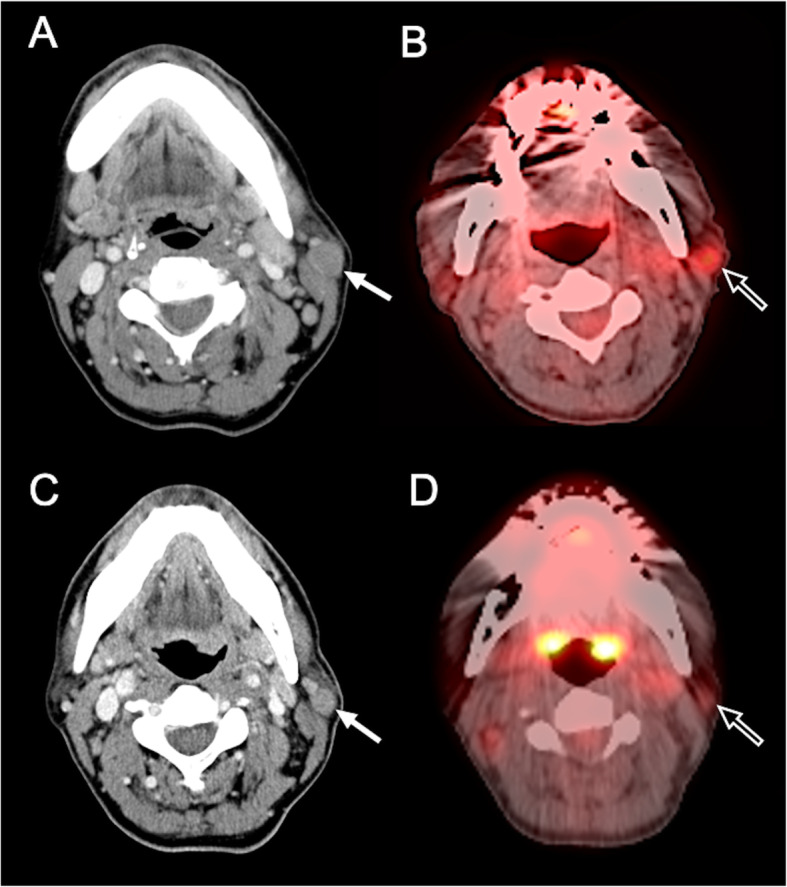
Response Evaluation Criteria in Solid Tumors (RECIST) is the gold standard for assessment of treatment response in solid tumors. Morphologic change of tumor size evaluated by RECIST is often correlated with survival length and has been considered as a surrogate endpoint of therapeutic efficacy. However, the detection of morphologic change alone may not be sufficient for assessing response to new anti-cancer medication in all solid tumors. During the past fifteen years, several molecular-targeted therapies and immunotherapies have emerged in cancer treatment which work by disrupting signaling pathways and inhibited cell growth. Tumor necrosis or lack of tumor progression is associated with a good therapeutic response even in the absence of tumor shrinkage. Therefore, the use of unmodified RECIST criteria to estimate morphological changes of tumor alone may not be sufficient to estimate tumor response for these new anti-cancer drugs. Several studies have reported the low reliability of RECIST in evaluating treatment response in different tumors such as hepatocellular carcinoma, lung cancer, prostate cancer, brain glioma, bone metastasis, and lymphoma. There is an increased need for new medical imaging biomarkers, considering the changes in tumor viability, metabolic activity, and attenuation, which are related to early tumor response. Promising imaging techniques, beyond RECIST, include dynamic contrast-enhanced computed tomography (CT) or magnetic resonance imaging (MRI), diffusion-weight imaging (DWI), magnetic resonance spectroscopy (MRS), and 18 F-fluorodeoxyglucose (FDG) positron emission tomography (PET). This review outlines the current RECIST with their limitations and the new emerging concepts of imaging biomarkers in oncology.
Keywords: Imaging biomarker; RECIST; Tumor response.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Therasse P, Arbuck SG, Eisenhauer EA, Wanders J, Kaplan RS, Rubinstein L, et al. New guidelines to evaluate the response to treatment in solid tumors. European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada. J Natl Cancer Inst. 2000;92(3):205–16. doi: 10.1093/jnci/92.3.205. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
