

India's pragmatic vaccination strategy against COVID-19: a mathematical modelling-based analysis
- PMID: 34215611
- PMCID: PMC8257292
- DOI: 10.1136/bmjopen-2021-048874
India's pragmatic vaccination strategy against COVID-19: a mathematical modelling-based analysis
Abstract
Objectives: To investigate the impact of targeted vaccination strategies on morbidity and mortality due to COVID-19, as well as on the incidence of SARS-CoV-2, in India.
Design: Mathematical modelling.
Settings: Indian epidemic of COVID-19 and vulnerable population.
Data sources: Country-specific and age-segregated pattern of social contact, case fatality rate and demographic data obtained from peer-reviewed literature and public domain.
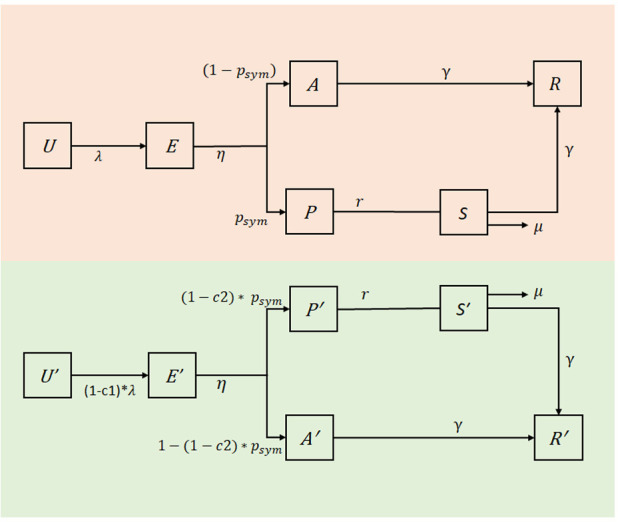
Model: An age-structured dynamical model describing SARS-CoV-2 transmission in India incorporating uncertainty in natural history parameters was constructed.
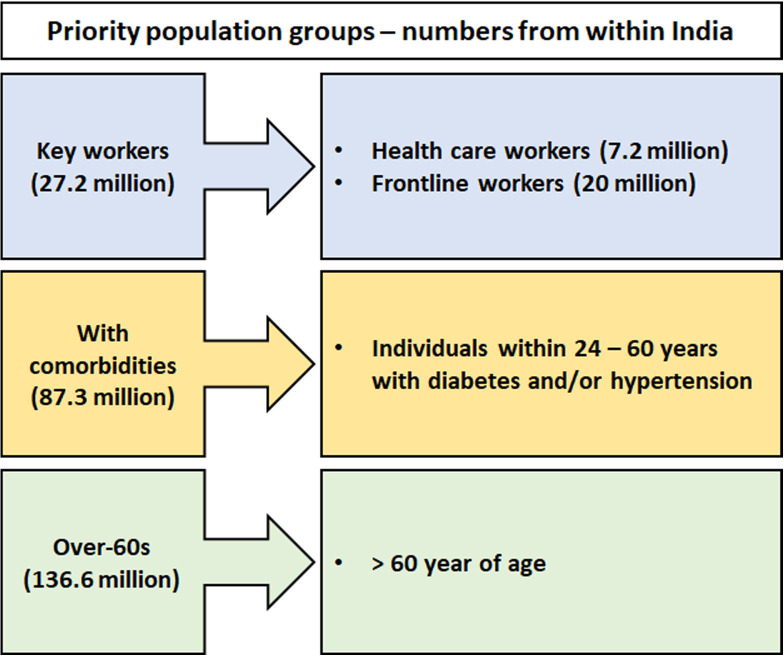
Interventions: Comparison of different vaccine strategies by targeting priority groups such as keyworkers including healthcare professionals, individuals with comorbidities (24-60 years old) and all above 60.
Main outcome measures: Incidence reduction and averted deaths in different scenarios, assuming that the current restrictions are fully lifted as vaccination is implemented.
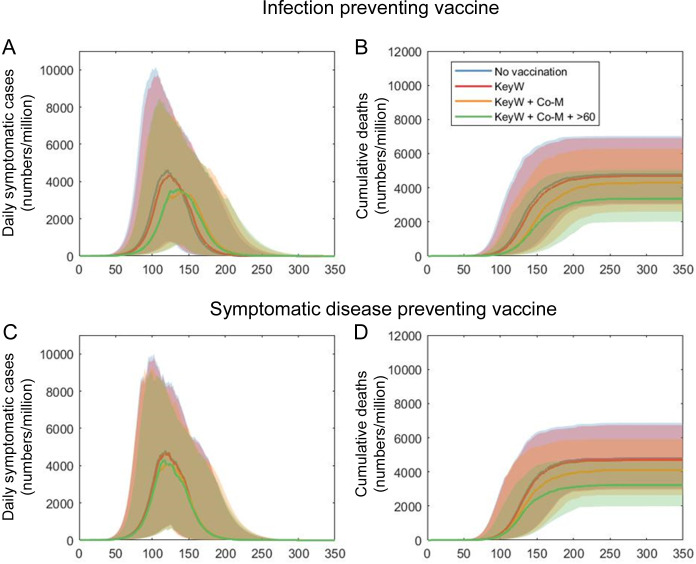
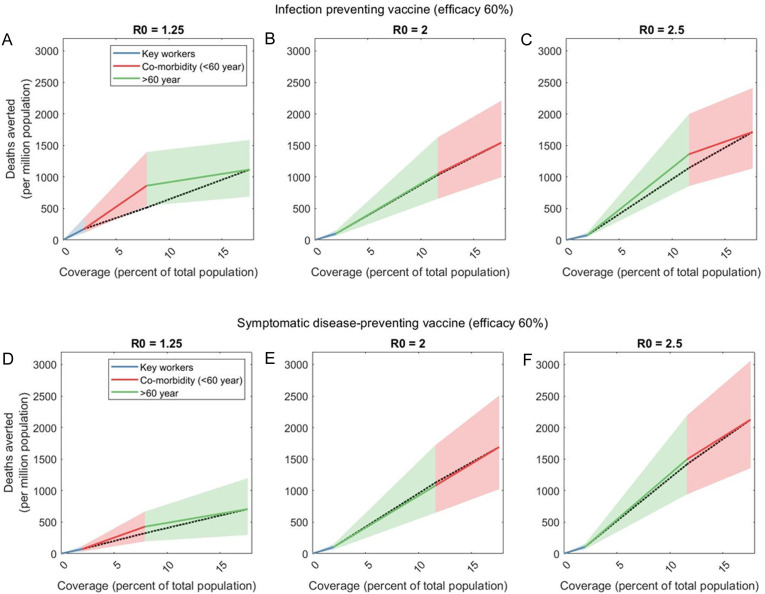
Results: The priority groups together account for about 18% of India's population. An infection-preventing vaccine with 60% efficacy covering all these groups would reduce peak symptomatic incidence by 20.6% (95% uncertainty intervals (UI) 16.7-25.4) and cumulative mortality by 29.7% (95% CrI 25.8-33.8). A similar vaccine with ability to prevent symptoms (but not infection) will reduce peak incidence of symptomatic cases by 10.4% (95% CrI 8.4-13.0) and cumulative mortality by 32.9% (95% CrI 28.6-37.3). In the event of insufficient vaccine supply to cover all priority groups, model projections suggest that after keyworkers, vaccine strategy should prioritise all who are >60 and subsequently individuals with comorbidities. In settings with weakest transmission, such as sparsely populated rural areas, those with comorbidities should be prioritised after keyworkers.
Conclusions: An appropriately targeted vaccination strategy would witness substantial mitigation of impact of COVID-19 in a country like India with wide heterogeneity. 'Smart vaccination', based on public health considerations, rather than mass vaccination, appears prudent.
Keywords: COVID-19; epidemiology; health policy; public health.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous