

Determinants of response to daratumumab in Epstein-Barr virus-positive natural killer and T-cell lymphoma
- PMID: 34215687
- PMCID: PMC8256838
- DOI: 10.1136/jitc-2020-002123
Determinants of response to daratumumab in Epstein-Barr virus-positive natural killer and T-cell lymphoma
Abstract
Background: The potential therapeutic efficacy of daratumumab in natural killer T-cell lymphoma (NKTL) was highlighted when its off-label usage produced sustained remission in a patient with highly refractory disease. This is corroborated recently by a phase II clinical trial which established that daratumumab monotherapy is well tolerated and displayed encouraging response in relapsed/refractory NKTL patients. However, little is known regarding the molecular factors central to the induction and regulation of the daratumumab-mediated antitumor response in NKTL.
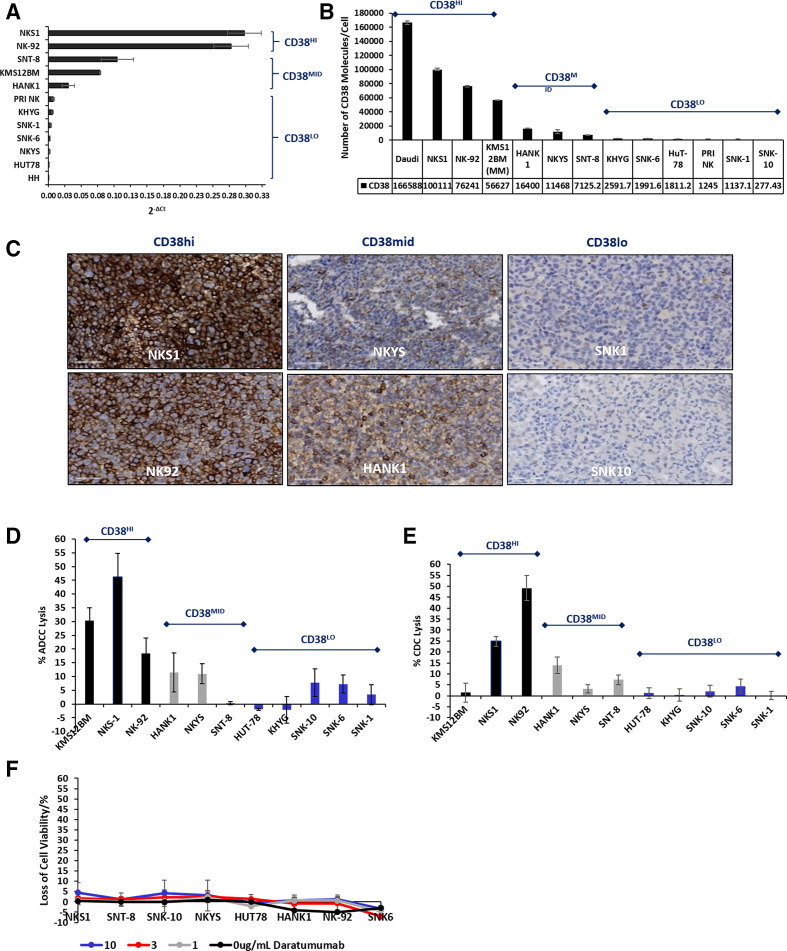
Methods: CD38 expression was studied via immunohistochemistry, multiplex immunofluorescence and correlated with clinical characteristics of the patient. The therapeutic efficacy of daratumumab was studied in vitro via CellTiter-Glo (CTG) assay, complement-dependent cytotoxicity (CDC), antibody-dependent cell cytotoxicity (ADCC), and in vivo, via a patient-derived xenograft mouse model of NKTL, both as a single agent and in combination with L-asparaginase. Signaling mechanisms were characterized via pharmacologic treatment, RNA silencing, flow cytometry and corroborated with public transcriptomic data of NKTL.
Results: Epstein-Barr virus-positive NKTL patients significantly express CD38 with half exhibiting high expression. Daratumumab effectively triggers Fc-mediated ADCC and CDC in a CD38-dependent manner. Importantly, daratumumab monotherapy and combination therapy with L-asparaginase significantly suppresses tumor progression in vivo. Ablation of complement inhibitory proteins (CIP) demonstrate that CD55 and CD59, not CD46, are critical for the induction of CDC. Notably, CD55 and CD59 expression were significantly elevated in the late stages of NKTL. Increasing the CD38:CIP ratio through sequential CIP knockdown, followed by CD38 upregulation via All-Trans Retinoic Acid treatment, potently augments complement-mediated lysis in cells previously resistant to daratumumab. The CD38:CIP ratio consistently demonstrates a statistically superior correlation to antitumor efficacy of daratumumab than CD38 or CIP expression alone.
Conclusion: This study characterizes CD38 as an effective target for a subset of NKTL patients and the utilization of the CD38:CIP ratio as a more robust identifier for patient stratification and personalisation of treatment. Furthermore, elucidation of factors which sensitize the complement-mediated response provides an alternative approach toward optimizing therapeutic efficacy of daratumumab where CDC remains a known limiting factor. Altogether, these results propose a strategic rationale for further evaluation of single or combined daratumumab treatment in the clinic for NKTL.
Keywords: antibodies; drug evaluation; hematologic neoplasms; immunotherapy; neoplasm; preclinical.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: LZ and JY are staff of Janssen Pharmaceuticals.
Figures





References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous