

Computer-aided interpretation of chest radiography reveals the spectrum of tuberculosis in rural South Africa
- PMID: 34215836
- PMCID: PMC8253848
- DOI: 10.1038/s41746-021-00471-y
Computer-aided interpretation of chest radiography reveals the spectrum of tuberculosis in rural South Africa
Erratum in
-
Publisher Correction: Computer-aided interpretation of chest radiography reveals the spectrum of tuberculosis in rural South Africa.NPJ Digit Med. 2021 Jul 16;4(1):115. doi: 10.1038/s41746-021-00485-6. NPJ Digit Med. 2021. PMID: 34272478 Free PMC article. No abstract available.
Abstract
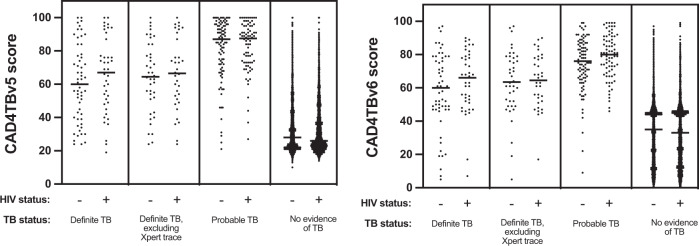
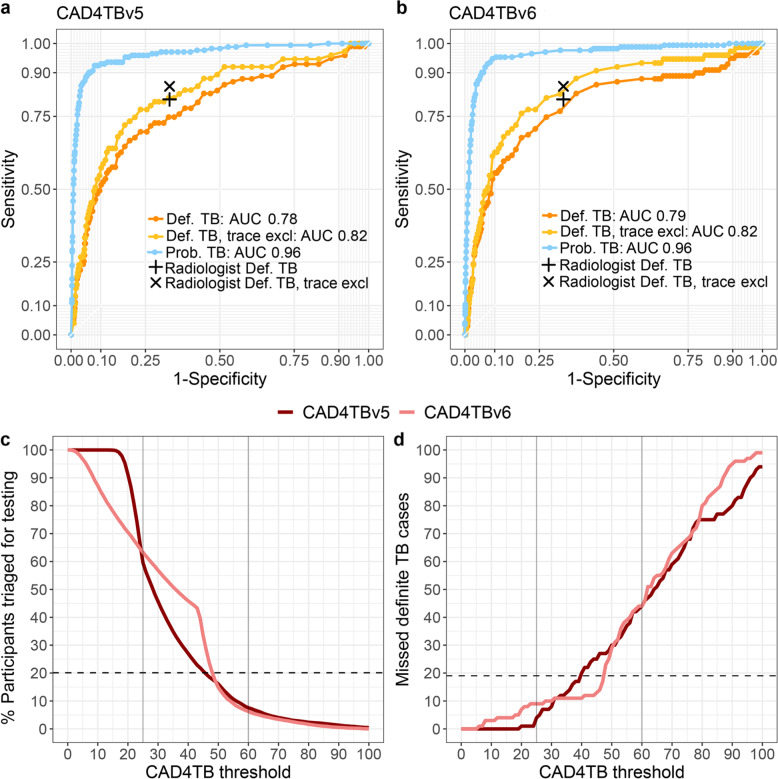
Computer-aided digital chest radiograph interpretation (CAD) can facilitate high-throughput screening for tuberculosis (TB), but its use in population-based active case-finding programs has been limited. In an HIV-endemic area in rural South Africa, we used a CAD algorithm (CAD4TBv5) to interpret digital chest x-rays (CXR) as part of a mobile health screening effort. Participants with TB symptoms or CAD4TBv5 score above the triaging threshold were referred for microbiological sputum assessment. During an initial pilot phase, a low CAD4TBv5 triaging threshold of 25 was selected to maximize TB case finding. We report the performance of CAD4TBv5 in screening 9,914 participants, 99 (1.0%) of whom were found to have microbiologically proven TB. CAD4TBv5 was able to identify TB cases at the same sensitivity but lower specificity as a blinded radiologist, whereas the next generation of the algorithm (CAD4TBv6) achieved comparable sensitivity and specificity to the radiologist. The CXRs of people with microbiologically confirmed TB spanned a range of lung field abnormality, including 19 (19.2%) cases deemed normal by the radiologist. HIV serostatus did not impact CAD4TB's performance. Notably, 78.8% of the TB cases identified during this population-based survey were asymptomatic and therefore triaged for sputum collection on the basis of CAD4TBv5 score alone. While CAD4TBv6 has the potential to replace radiologists for triaging CXRs in TB prevalence surveys, population-specific piloting is necessary to set the appropriate triaging thresholds. Further work on image analysis strategies is needed to identify radiologically subtle active TB.
Conflict of interest statement
We declare no competing financial or non-financial interests. CAD4TBv5 scores were purchased from Delft but CAD4TBv6 scores were provided free of charge. Delft did not contribute any funding and was not involved in the analysis and writing of the report.
Figures


References
-
- World Health Organization (WHO). WHO End TB Strategy. https://www.who.int/tb/strategy/en/ (2015).
-
- Corbett EL, et al. Comparison of two active case-finding strategies for community-based diagnosis of symptomatic smear-positive tuberculosis and control of infectious tuberculosis in Harare, Zimbabwe (DETECTB): a cluster-randomised trial. Lancet. 2010;376:1244–1253. doi: 10.1016/S0140-6736(10)61425-0. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
