

Validation of a liquid biopsy assay with molecular and clinical profiling of circulating tumor DNA
- PMID: 34215841
- PMCID: PMC8253837
- DOI: 10.1038/s41698-021-00202-2
Validation of a liquid biopsy assay with molecular and clinical profiling of circulating tumor DNA
Abstract
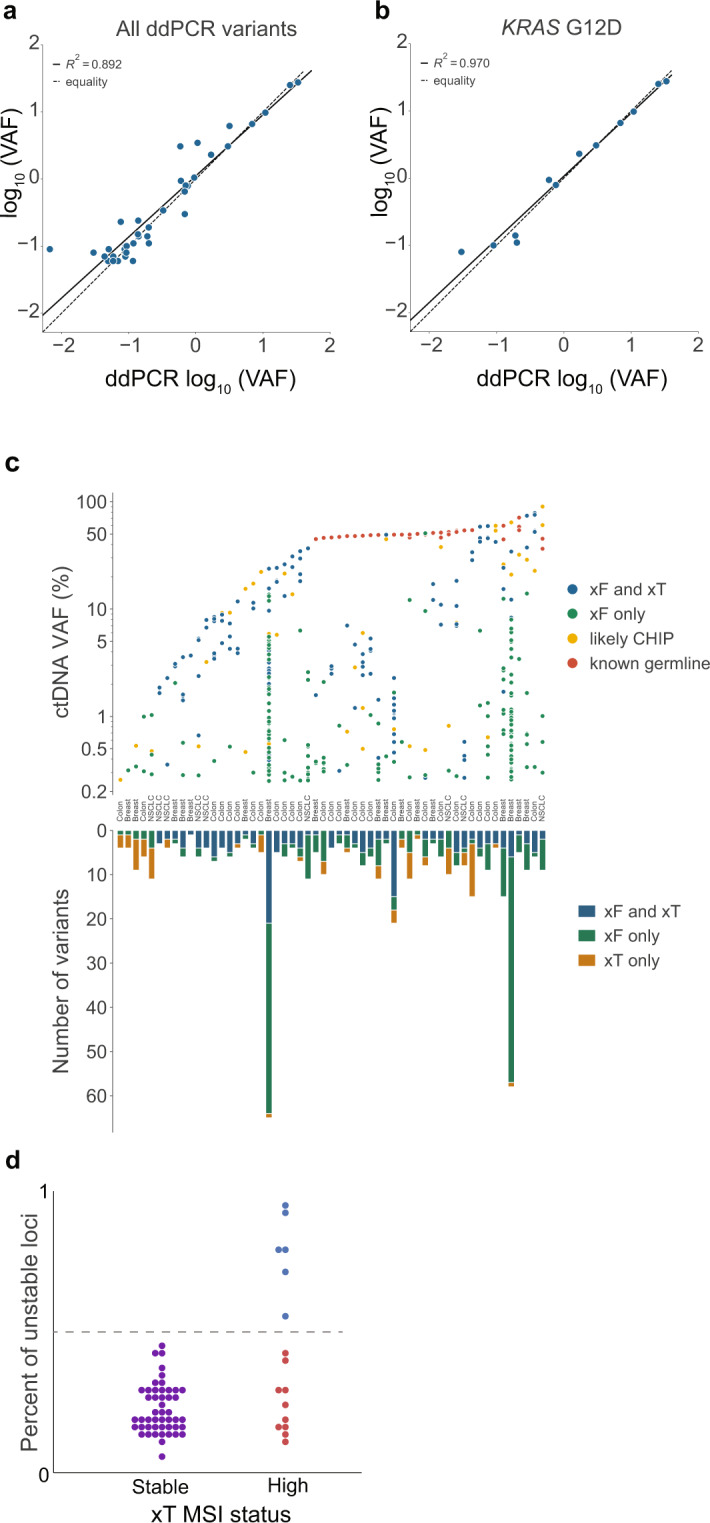
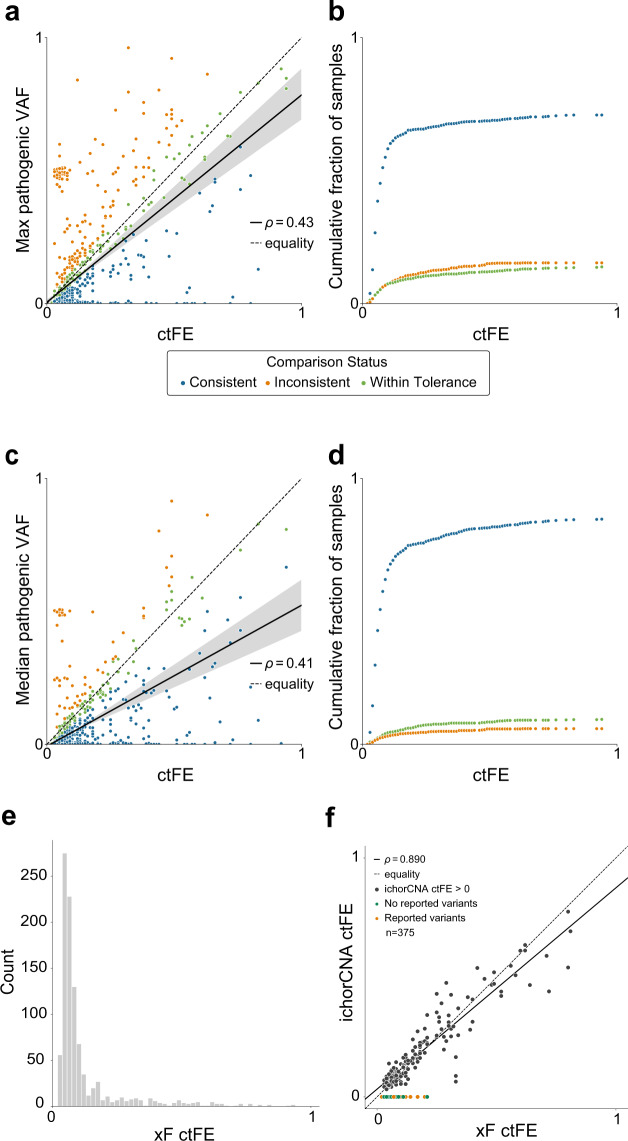
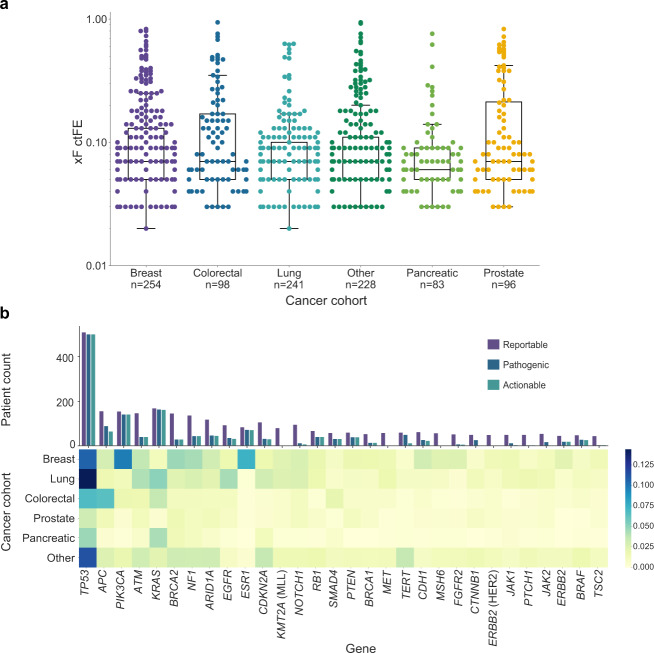
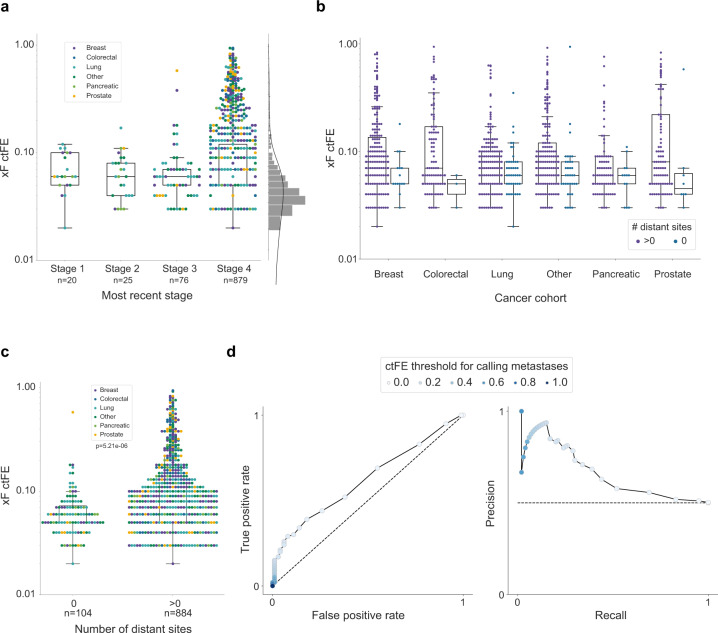
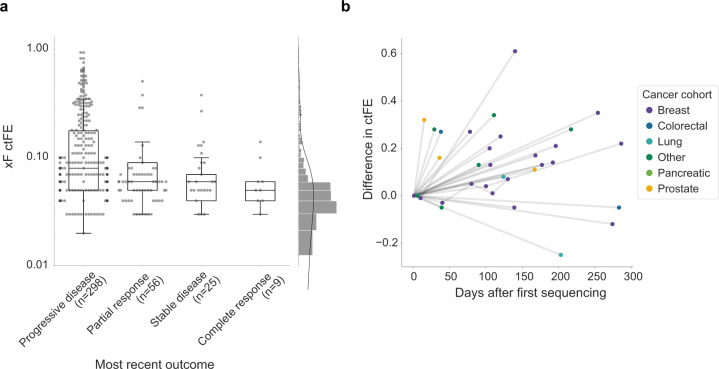
Liquid biopsy is a valuable precision oncology tool that is increasingly used as a non-invasive approach to identify biomarkers, detect resistance mutations, monitor disease burden, and identify early recurrence. The Tempus xF liquid biopsy assay is a 105-gene, hybrid-capture, next-generation sequencing (NGS) assay that detects single-nucleotide variants, insertions/deletions, copy number variants, and chromosomal rearrangements. Here, we present extensive validation studies of the xF assay using reference standards, cell lines, and patient samples that establish high sensitivity, specificity, and accuracy in variant detection. The Tempus xF assay is highly concordant with orthogonal methods, including ddPCR, tumor tissue-based NGS assays, and another commercial plasma-based NGS assay. Using matched samples, we developed a dynamic filtering method to account for germline mutations and clonal hematopoiesis, while significantly decreasing the number of false-positive variants reported. Additionally, we calculated accurate circulating tumor fraction estimates (ctFEs) using the Off-Target Tumor Estimation Routine (OTTER) algorithm for targeted-panel sequencing. In a cohort of 1,000 randomly selected cancer patients who underwent xF testing, we found that ctFEs correlated with disease burden and clinical outcomes. These results highlight the potential of serial testing to monitor treatment efficacy and disease course, providing strong support for incorporating liquid biopsy in the management of patients with advanced disease.
Conflict of interest statement
J.D.F., H.B., T.M.D., C.L., R.A.B., A.H., A.A.K., A.L., K.E.M., J.P., W.Z., K.P.W., R.T. and N.B are employees and shareholders of Tempus Labs, Inc. The remaining authors declare no competing interests.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
