

Cardiovascular Toxicity of Androgen Deprivation Therapy
- PMID: 34216282
- PMCID: PMC8254069
- DOI: 10.1007/s11886-021-01561-9
Cardiovascular Toxicity of Androgen Deprivation Therapy
Abstract
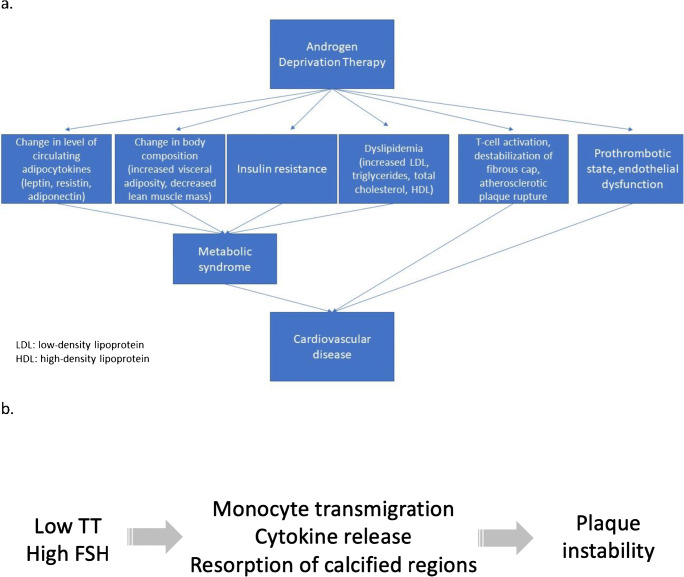
Purpose of review: Androgen deprivation therapy (ADT) is the standard of care for the treatment of advanced prostate cancer (PC). ADT, particularly with GnRH agonists, leads to increased risk of cardiovascular disease, including myocardial infarction, hypertension, and stroke. This review discusses the options of ADT, the mechanism of ADT-associated cardiovascular side effects, and potential benefit by using GnRH antagonists.
Recent findings: GnRH antagonists have relatively less cardiovascular adverse effects compared to GnRH agonists. We highlight on a recently published phase III clinical trial on the oral GnRH antagonist, relugolix, and its comparative benefit to traditional GnRH agonist regarding development of cardiovascular disease. Recent data reinforces that GnRH antagonists have a more favorable cardiovascular outcomes compared to GnRH agonists yet maintain a similar efficacy profile. From the data we reviewed, GnRH antagonists may be the preferred method of ADT for PC, but further data with primary cardiovascular outcomes are warranted.
Keywords: Androgen deprivation therapy; Cardio-oncology; Cardiovascular toxicity; Coronary artery disease; GnRH antagonist; Prostate cancer.
Conflict of interest statement
The authors have no conflict of interest to report.
Figures
References
-
- Bekelman JE, Rumble RB, Chen RC, Pisansky TM, Finelli A, Feifer A, Nguyen PL, Loblaw DA, Tagawa ST, Gillessen S, Morgan TM, Liu G, Vapiwala N, Haluschak JJ, Stephenson A, Touijer K, Kungel T, Freedland SJ. Clinically localized prostate cancer: ASCO clinical practice guideline endorsement of an American Urological Association/American Society for Radiation Oncology/Society of Urologic Oncology Guideline. J Clin Oncol. 2018;36(32):3251–3258. doi: 10.1200/JCO.18.00606. - DOI - PubMed
-
- Maximum androgen blockade in advanced prostate cancer: an overview of the randomised trials. Prostate Cancer Trialists' Collaborative Group. Lancet, 2000. 355(9214): p. 1491-8. - PubMed
-
- Bhatia N, Santos M, Jones LW, Beckman JA, Penson DF, Morgans AK, Moslehi J. Cardiovascular effects of androgen deprivation therapy for the treatment of prostate cancer: ABCDE steps to reduce cardiovascular disease in patients with prostate cancer. Circulation. 2016;133(5):537–541. doi: 10.1161/CIRCULATIONAHA.115.012519. - DOI - PMC - PubMed
-
- Knutsson A, Hsiung S, Celik S, Rattik S, Mattisson IY, Wigren M, Scher HI, Nilsson J, Hultgårdh-Nilsson A. Treatment with a GnRH receptor agonist, but not the GnRH receptor antagonist degarelix, induces atherosclerotic plaque instability in ApoE(-/-) mice. Sci Rep. 2016;6:26220. doi: 10.1038/srep26220. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
