

Pre-existing cardiovascular disease rather than cardiovascular risk factors drives mortality in COVID-19
- PMID: 34217220
- PMCID: PMC8254437
- DOI: 10.1186/s12872-021-02137-9
Pre-existing cardiovascular disease rather than cardiovascular risk factors drives mortality in COVID-19
Abstract
Background: The relative association between cardiovascular (CV) risk factors, such as diabetes and hypertension, established CV disease (CVD), and susceptibility to CV complications or mortality in COVID-19 remains unclear.
Methods: We conducted a cohort study of consecutive adults hospitalised for severe COVID-19 between 1st March and 30th June 2020. Pre-existing CVD, CV risk factors and associations with mortality and CV complications were ascertained.
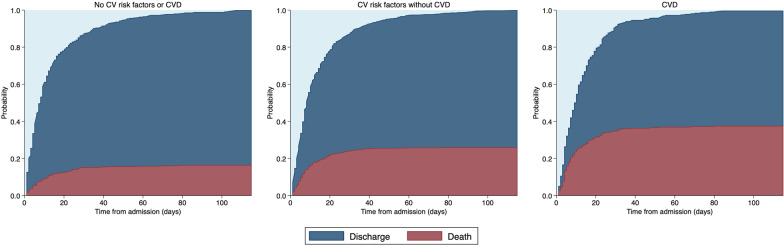
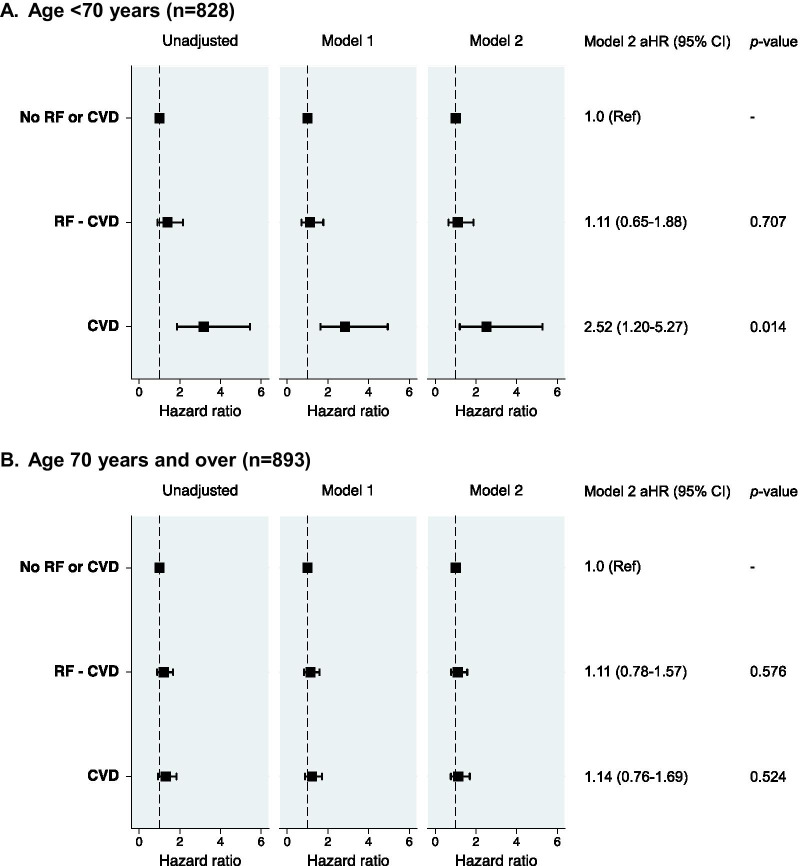
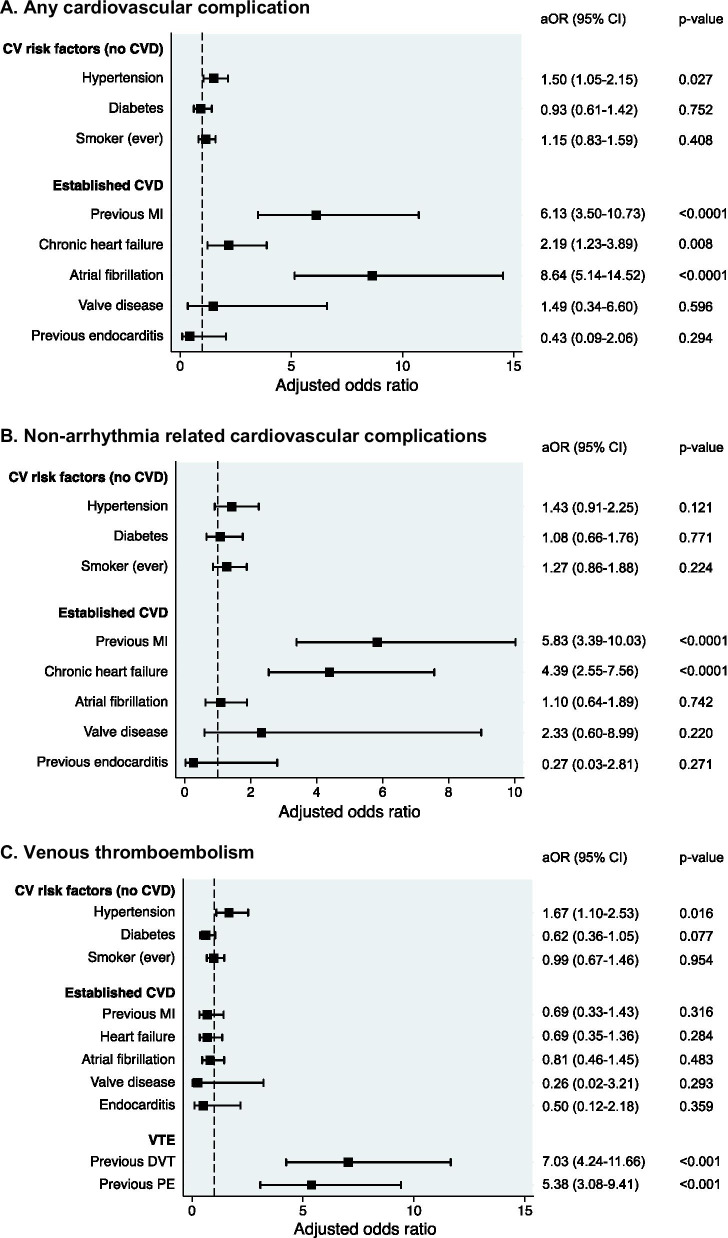
Results: Among 1721 patients (median age 71 years, 57% male), 349 (20.3%) had pre-existing CVD (CVD), 888 (51.6%) had CV risk factors without CVD (RF-CVD), 484 (28.1%) had neither. Patients with CVD were older with a higher burden of non-CV comorbidities. During follow-up, 438 (25.5%) patients died: 37% with CVD, 25.7% with RF-CVD and 16.5% with neither. CVD was independently associated with in-hospital mortality among patients < 70 years of age (adjusted HR 2.43 [95% CI 1.16-5.07]), but not in those ≥ 70 years (aHR 1.14 [95% CI 0.77-1.69]). RF-CVD were not independently associated with mortality in either age group (< 70 y aHR 1.21 [95% CI 0.72-2.01], ≥ 70 y aHR 1.07 [95% CI 0.76-1.52]). Most CV complications occurred in patients with CVD (66%) versus RF-CVD (17%) or neither (11%; p < 0.001). 213 [12.4%] patients developed venous thromboembolism (VTE). CVD was not an independent predictor of VTE.
Conclusions: In patients hospitalised with COVID-19, pre-existing established CVD appears to be a more important contributor to mortality than CV risk factors in the absence of CVD. CVD-related hazard may be mediated, in part, by new CV complications. Optimal care and vigilance for destabilised CVD are essential in this patient group. Trial registration n/a.
Keywords: COVID-19; Cardiovascular disease; Cardiovascular risk factors; Diabetes; Hypertension.
Conflict of interest statement
JTHT received research funding from Innovate UK & Office of Life Sciences, and iRhythm Technologies, and holds shares < £5,000 in Glaxo Smithkline and Biogen. The other authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
