

Inappropriate surgery in a patient with misdiagnosed Robert's uterus
- PMID: 34217289
- PMCID: PMC8254971
- DOI: 10.1186/s12905-021-01404-3
Inappropriate surgery in a patient with misdiagnosed Robert's uterus
Abstract
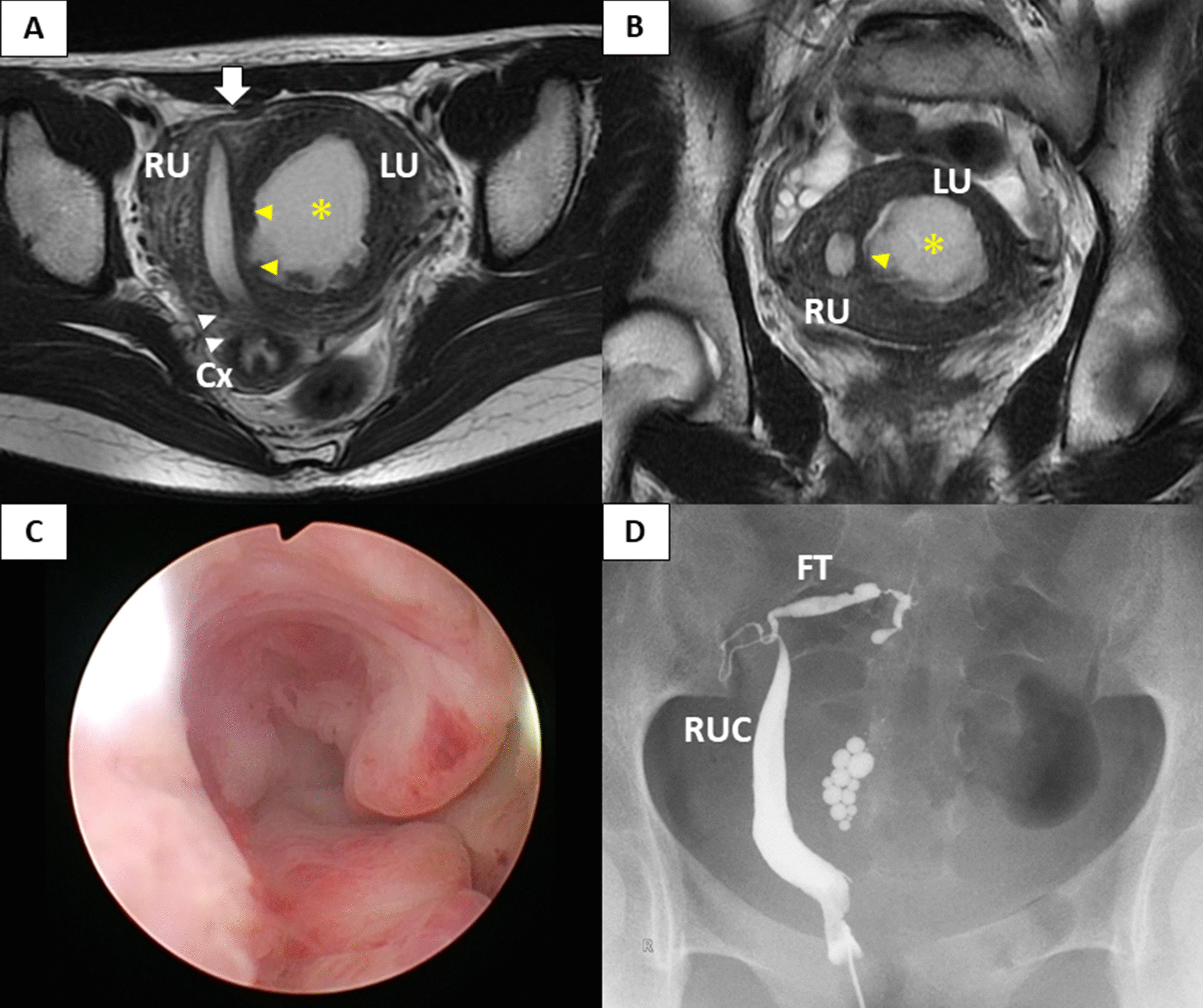
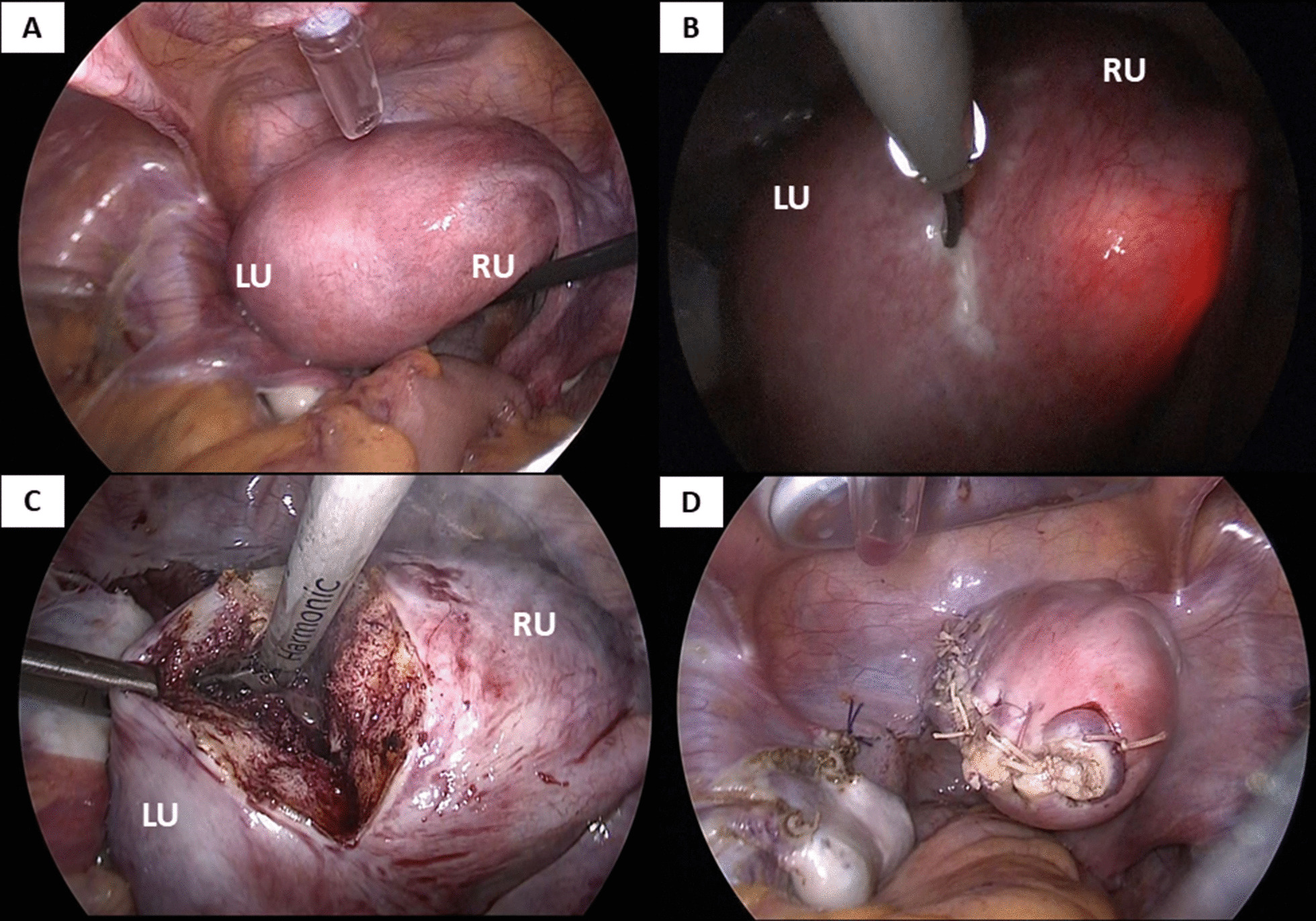
Background: Robert's uterus is a rare Mullerian anomaly, which can be described as an asymmetric, septate uterus with a non-communicating hemicavity. Herein, we present the case of a misdiagnosed Robert's uterus, resulting in an invasive and disadvantageous surgery.
Case presentation: A 16-year-old woman was referred to our department because of dysmenorrhea and suspicion of uterine malformation. We misdiagnosed Robert's uterus as a unicornuate uterus with a non-communicating rudimentary horn and hematometra, and performed laparoscopic hemi-hysterectomy. Although the patient's symptoms were relieved, our surgical procedure left the lateral uterine wall weak, making the patient's uterus susceptible to uterine rupture in any future pregnancy.
Conclusions: Although the early diagnosis of Robert's uterus is challenging, it is important in order to determine appropriate surgical interventions and management for maintaining the quality of life and ensuring safety in future pregnancies.
Keywords: Dysmenorrhea; Hematometra; Mullerian anomaly; Robert’s uterus; Rudimentary horn; Septate uterus; Unicornuate uterus.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Robert H. Asymmetrical bifidities with unilateral menstrual retention. Chirurgie. 1970;96:796–9. - PubMed
-
- Di Spiezio Sardo A, Giampaolino P, Scognamiglio M, Varelli C, Nazzaro G, Mansueto G, et al. An exceptional case of complete septate uterus with unilateral cervical aplasia (Class U2bC3V0/ESHRE/ESGE classification) and isolated Mullerian remnants: combined hysteroscopic and laparoscopic treatment. J Minim Invasive Gynecol. 2016;23:16–7. doi: 10.1016/j.jmig.2015.09.006. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
