

Robot-mediated overground gait training for transfemoral amputees with a powered bilateral hip orthosis: a pilot study
- PMID: 34217307
- PMCID: PMC8254913
- DOI: 10.1186/s12984-021-00902-7
Robot-mediated overground gait training for transfemoral amputees with a powered bilateral hip orthosis: a pilot study
Abstract
Background: Transfemoral amputation is a serious intervention that alters the locomotion pattern, leading to secondary disorders and reduced quality of life. The outcomes of current gait rehabilitation for TFAs seem to be highly dependent on factors such as the duration and intensity of the treatment and the age or etiology of the patient. Although the use of robotic assistance for prosthetic gait rehabilitation has been limited, robotic technologies have demonstrated positive rehabilitative effects for other mobility disorders and may thus offer a promising solution for the restoration of healthy gait in TFAs. This study therefore explored the feasibility of using a bilateral powered hip orthosis (APO) to train the gait of community-ambulating TFAs and the effects on their walking abilities.
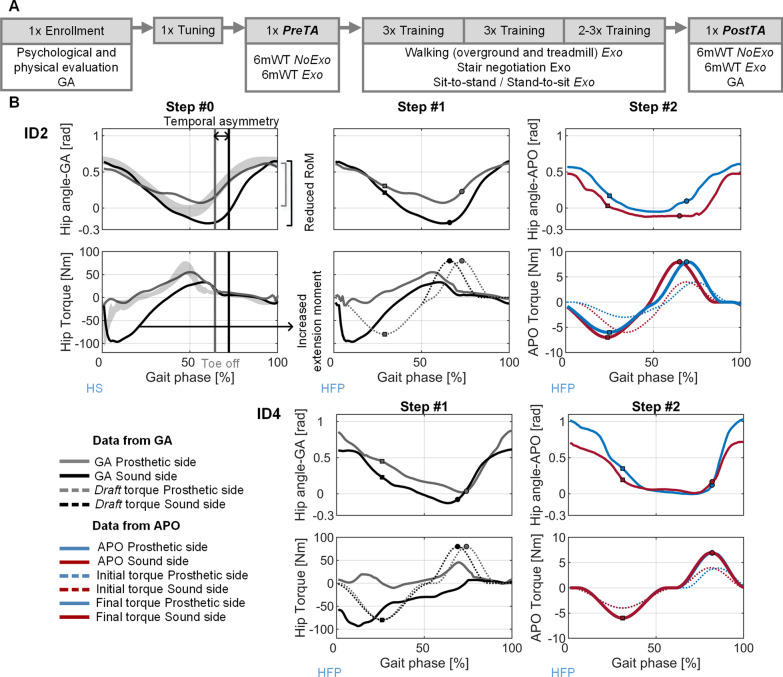
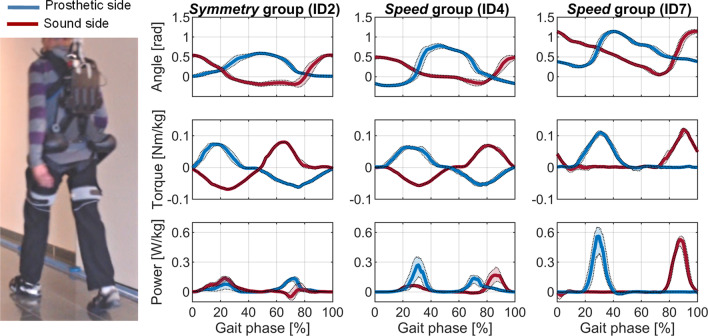
Methods: Seven participants (46-71 years old with different mobility levels) were included in the study and assigned to one of two groups (namely Symmetry and Speed groups) according to their prosthesis type, mobility level, and prior experience with the exoskeleton. Each participant engaged in a maximum of 12 sessions, divided into one Enrollment session, one Tuning session, two Assessment sessions (conducted before and after the training program), and eight Training sessions, each consisting of 20 minutes of robotically assisted overground walking combined with additional tasks. The two groups were assisted by different torque-phase profiles, aiming at improving symmetry for the Symmetry group and at maximizing the net power transferred by the APO for the Speed group. During the Assessment sessions, participants performed two 6-min walking tests (6mWTs), one with (Exo) and one without (NoExo) the exoskeleton, at either maximal (Symmetry group) or self-selected (Speed group) speed. Spatio-temporal gait parameters were recorded by commercial measurement equipment as well as by the APO sensors, and metabolic efficiency was estimated via the Cost of Transport (CoT). Additionally, kinetic and kinematic data were recorded before and after treatment in the NoExo condition.
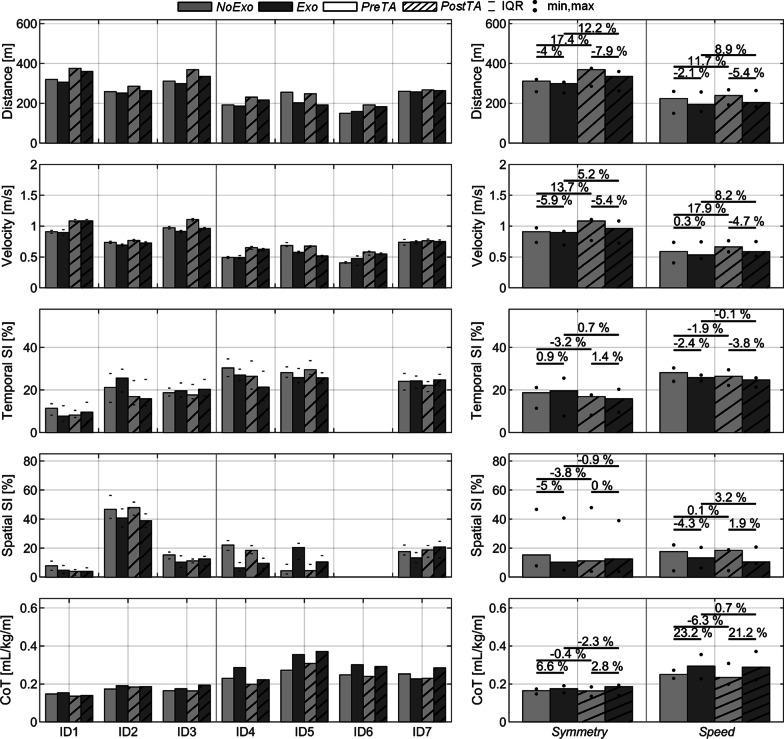
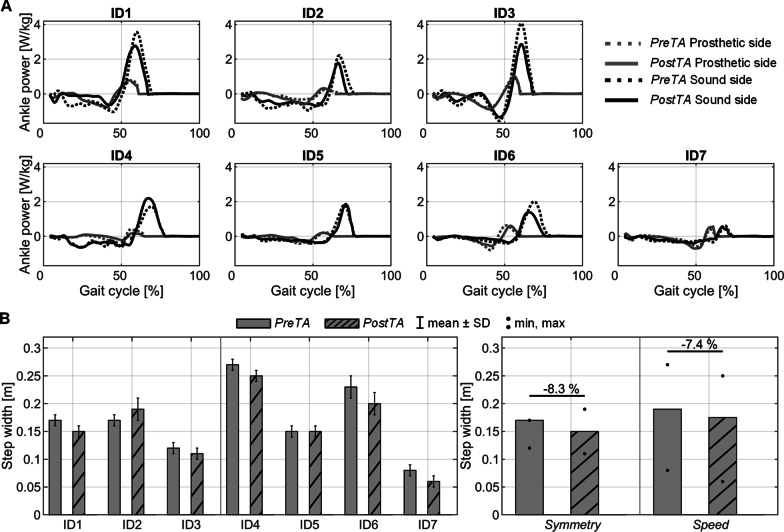
Results: The one-month training protocol was found to be a feasible strategy to train TFAs, as all participants smoothly completed the clinical protocol with no relevant mechanical failures of the APO. The walking performance of participants improved after the training. During the 6mWT in NoExo, participants in the Symmetry and Speed groups respectively walked 17.4% and 11.7% farther and increased walking speed by 13.7% and 17.9%, with improved temporal and spatial symmetry for the former group and decreased energetic expenditure for the latter. Gait analysis showed that ankle power, step width, and hip kinematics were modified towards healthy reference levels in both groups. In the Exo condition metabolic efficiency was reduced by 3% for the Symmetry group and more than 20% for the Speed group.
Conclusions: This study presents the first pilot study to apply a wearable robotic orthosis (APO) to assist TFAs in an overground gait rehabilitation program. The proposed APO-assisted training program was demonstrated as a feasible strategy to train TFAs in a rehabilitation setting. Subjects improved their walking abilities, although further studies are required to evaluate the effectiveness of the APO compared to other gait interventions. Future protocols will include a lighter version of the APO along with optimized assistive strategies.
Keywords: Exoskeleton; Gait rehabilitation; Gait training; Hip orthosis; Overground walking; Transfemoral amputees.
Conflict of interest statement
AP, RC, FG, SC and NV have interests in IUVO S.r.l. NV is a member of the Board of Directors and serves as Business Development and Innovation Advisor; SC is a Scientific Advisor. Part of the IP covering the technology presented in this paper has been exclusively licensed to IUVO for commercial exploitation. ÞF. and DR. are employed by Össur hf, which licenses IP related to the technology presented from IUVO S.r.l.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
