

Current Understanding and Future Perspectives of Interstitial Cystitis/Bladder Pain Syndrome
- PMID: 34218637
- PMCID: PMC8255826
- DOI: 10.5213/inj.2142084.042
Current Understanding and Future Perspectives of Interstitial Cystitis/Bladder Pain Syndrome
Abstract
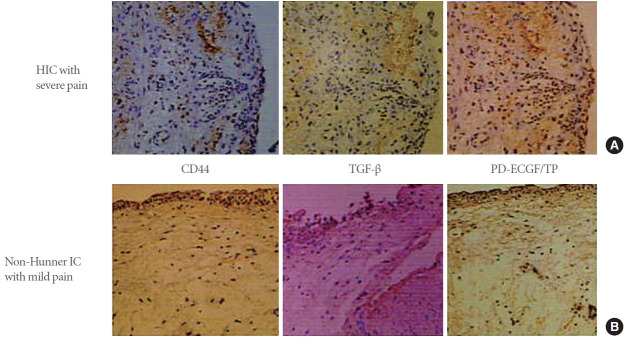
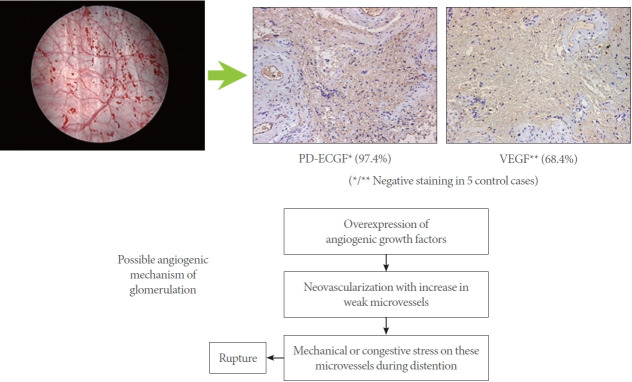
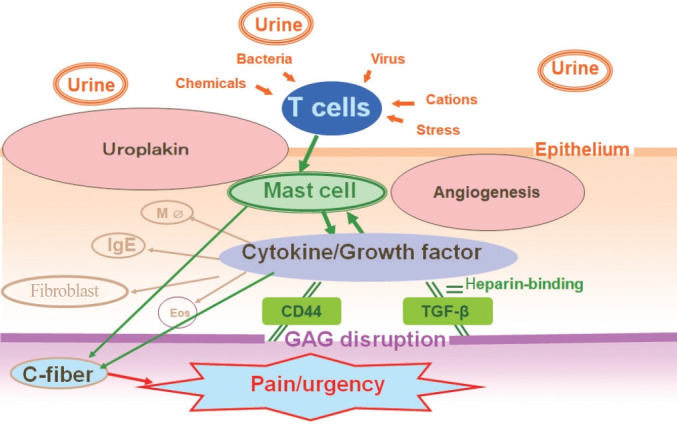
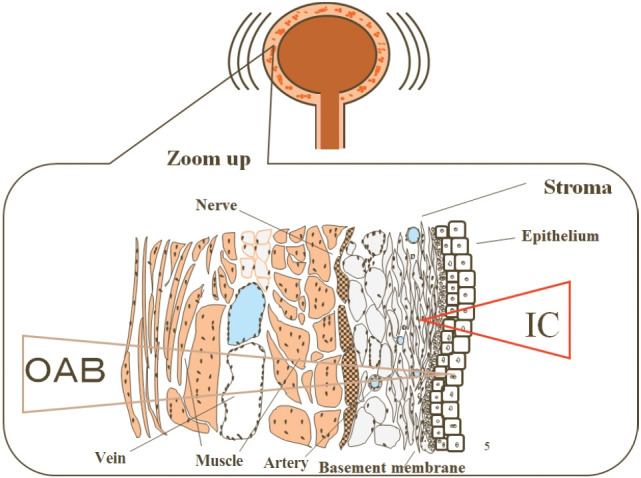
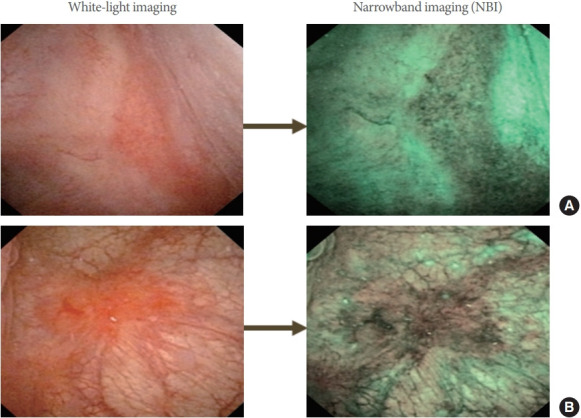
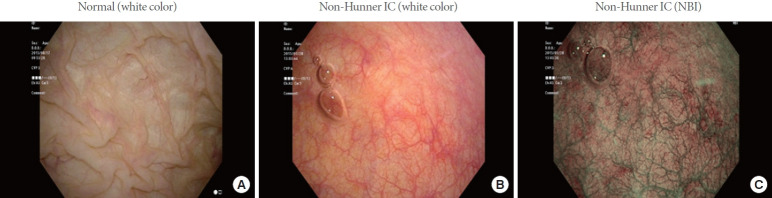
Interstitial cystitis/bladder pain syndrome (IC/BPS) is a chronic disease characterized by suprapubic pain and lower urinary tract symptoms. Perhaps because of the heterogeneous nature of this disease and its multifactorial etiology, clinical trials in allinclusive populations of IC/BPS patients without phenotyping in the last decade have mainly failed to discover new therapeutic modalities of IC/BPS. Thus, phenotyping IC/BPS, aimed at identifying bladder-centric and/or bladder-beyond pathologies, including cystoscopic observation of Hunner or non-Hunner lesions of the bladder mucosa, is particularly important for the future of IC/BPS management. Based on recent discussions at international conferences, including the International Consultation on IC, Japan, it has been proposed that Hunner-lesion IC should be separated from other non-Hunner IC/BPS because of its distinct inflammatory profiles and epithelial denudation compared with non-Hunner IC/BPS. However, there are still no standard criteria for the diagnosis of Hunner lesions other than typical lesions, while conventional cystoscopic observations may miss atypical or small Hunner lesions. Furthermore, diagnosis of the bladder-centric phenotype of IC/BPS requires confirmation that identified mucosal lesions are truly a cause of bladder pain in IC/BPS patients. This review article discusses the current status of IC/BPS pathophysiology and diagnosis, as well as future directions of the proper diagnosis of bladder-centric IC/BPS, in which pathophysiological mechanisms other than those in inflammatory pathways, such as angiogenic and immunogenic abnormalities, could also be involved in both Hunner-lesion IC and non-Hunner IC/BPS. It is hoped that this new paradigm in the pathophysiological evaluation and diagnosis of IC/BPS could lead to pathology-based phenotyping and new treatments for this heterogeneous disease.
Keywords: Angiogenesis; Bladder pain syndrome; Cystoscopy; Hunner lesion; Interstitial cystitis; Narrow-band imaging.
Conflict of interest statement
T. Ueda reports personal fees from Kyorin, Seikagaku and Japan Tobacco. P.M. Hanno has reports personal fees from Seikagaku, Ironwood, Imbrium, and HTL Biotech. N. Yoshimura reports personal fees from Kyorin and Astellas. R. Saito and J.M. Meijlink report no competing interests.
Figures

Comment in
-
Interstitial Cystitis: A Consequence of Weakened Uterosacral Ligaments Failing to Support Visceral Plexuses and Bladder Stretch Receptors, and Therefore Potentially Curable?Int Neurourol J. 2022 Dec;26(4):349-351. doi: 10.5213/inj.2142366.183. Epub 2022 Dec 30. Int Neurourol J. 2022. PMID: 36599344 Free PMC article. No abstract available.
-
Reply to "Interstitial Cystitis - A Consequence of Weakened Uterosacral Ligaments Failing to Support Visceral Plexuses and Bladder Stretch Receptors and Therefore Potentially Curable?".Int Neurourol J. 2022 Dec;26(4):352. doi: 10.5213/inj.2142204.102. Epub 2022 Dec 30. Int Neurourol J. 2022. PMID: 36599345 Free PMC article. No abstract available.
References
-
- Hunner G. A rare type of bladder ulcer in women; report of cases. Boston Med Surg J. 1915;172:660–4.
-
- Fall M, Logadottir Y, Peeker R. Interstitial cystitis is bladder pain syndrome with Hunner’s lesion. Int J Urol. 2014;21 Suppl 1:79–82. - PubMed
-
- Homma Y, Ueda T, Ito T, Takei M, Tomoe H. Japanese guideline for diagnosis and treatment of interstitial cystitis. Int J Urol. 2009;16:4–16. - PubMed
-
- Ogawa T, Ishizuka O, Ueda T, Tyagi P, Chancellor MB, Yoshimura N. Current and emerging drugs for interstitial cystitis/bladder pain syndrome (IC/BPS) Expert Opin Emerg Drugs. 2015;20:555–70. - PubMed
LinkOut - more resources
Full Text Sources
