

Diabetes Mellitus Is Associated With Poor In-Hospital and Long-Term Outcomes in Young and Midlife Stroke Survivors
- PMID: 34219470
- PMCID: PMC8483482
- DOI: 10.1161/JAHA.120.019991
Diabetes Mellitus Is Associated With Poor In-Hospital and Long-Term Outcomes in Young and Midlife Stroke Survivors
Abstract
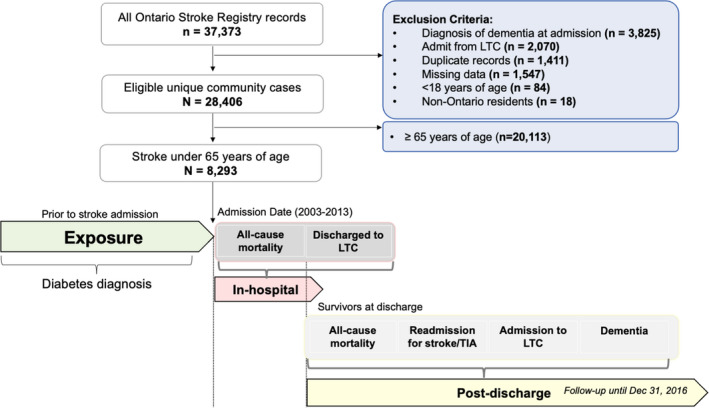
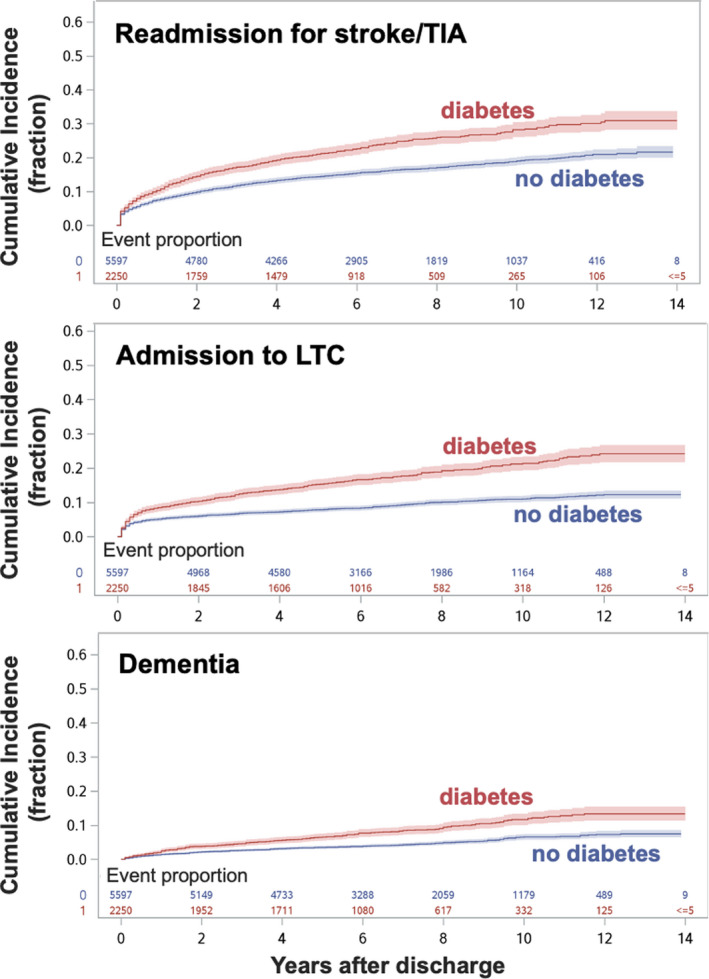
Background The incidence of ischemic stroke has increased among adults aged 18 to 64 years, yet little is known about relationships between specific risk factors and outcomes. This study investigates in-hospital and long-term outcomes in patients with stroke aged <65 years with preexisting diabetes mellitus. Methods and Results Consecutive patients aged <65 years admitted to comprehensive stroke centers for acute ischemic stroke between 2003 and 2013 were identified from the Ontario Stroke Registry. Multinomial logistic regression was used to estimate adjusted odds ratio (OR [95% CI]) of in-hospital mortality or direct discharge to long-term or continuing care. Cox proportional hazards regression was used to estimate the adjusted hazards ratio (aHR [95% CI]) of long-term mortality, readmission for stroke/transient ischemic attack, admission to long-term care, and incident dementia. Predefined sensitivity analyses examined stroke outcomes among young (aged 18-49 years) and midlife (aged 50-65 years) subgroups. Among 8293 stroke survivors (mean age, 53.6±8.9 years), preexisting diabetes mellitus was associated with a higher likelihood of in-hospital death (adjusted OR, 1.46 [95% CI, 1.14-1.87]) or direct discharge to long-term care (adjusted OR, 1.65 [95% CI, 1.07-2.54]). Among stroke survivors discharged (N=7847) and followed up over a median of 6.3 years, preexisting diabetes mellitus was associated with increased hazards of death (aHR, 1.68 [95% CI, 1.50-1.88]), admission to long-term care (aHR, 1.57 [95% CI, 1.35-1.82]), readmission for stroke/transient ischemic attack (aHR, 1.37 [95% CI, 0.21-1.54]), and incident dementia (aHR, 1.44 [95% CI, 1.17-1.77]). Only incident dementia was not increased for young stroke survivors. Conclusions Focused secondary prevention and risk factor management may be needed to address poor long-term outcomes for patients with stroke aged <65 years with preexisting diabetes mellitus.
Keywords: dementia; diabetes mellitus; ischemic; longitudinal; midlife; stroke; young.
Conflict of interest statement
J. Colby‐Milley (formerly of Sunnybrook Research Institute) is now a paid employee of F. Hoffmann‐La Roche Ltd (as of July 29, 2019), but their role is unrelated to the present work. The remaining authors have no disclosures to report.
Figures
References
-
- Kleindorfer DO, Khoury J, Moomaw CJ, Alwell K, Woo D, Flaherty ML, Khatri P, Adeoye O, Ferioli S, Broderick JP, et al. Stroke incidence is decreasing in whites but not in blacks: a population‐based estimate of temporal trends in stroke incidence from the Greater Cincinnati/Northern Kentucky stroke study. Stroke. 2010;41:1326–1331. DOI: 10.1161/STROKEAHA.109.575043. - DOI - PMC - PubMed
-
- Madsen TE, Khoury J, Alwell K, Moomaw CJ, Rademacher E, Flaherty ML, Woo D, Mackey J, De Los Rios La Rosa F, Martini S, et al. Sex‐specific stroke incidence over time in the Greater Cincinnati/Northern Kentucky Stroke Study. Neurology. 2017;89:990–996. DOI: 10.1212/WNL.0000000000004325. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
