

Impact of Arterial Remodeling of Intermediate Coronary Lesions on Long-Term Clinical Outcomes in Patients with Stable Coronary Artery Disease: An Intravascular Ultrasound Study
- PMID: 34220369
- PMCID: PMC8213497
- DOI: 10.1155/2021/9915759
Impact of Arterial Remodeling of Intermediate Coronary Lesions on Long-Term Clinical Outcomes in Patients with Stable Coronary Artery Disease: An Intravascular Ultrasound Study
Abstract
Background: Treatment of coronary intermediate lesions remains a controversy, and the role of arterial remodeling patterns determined by intravascular ultrasound in intermediate lesion is still not well known. The aim of this study was to investigate the impact of arterial remodeling of intermediate coronary lesions on long-term clinical outcomes.
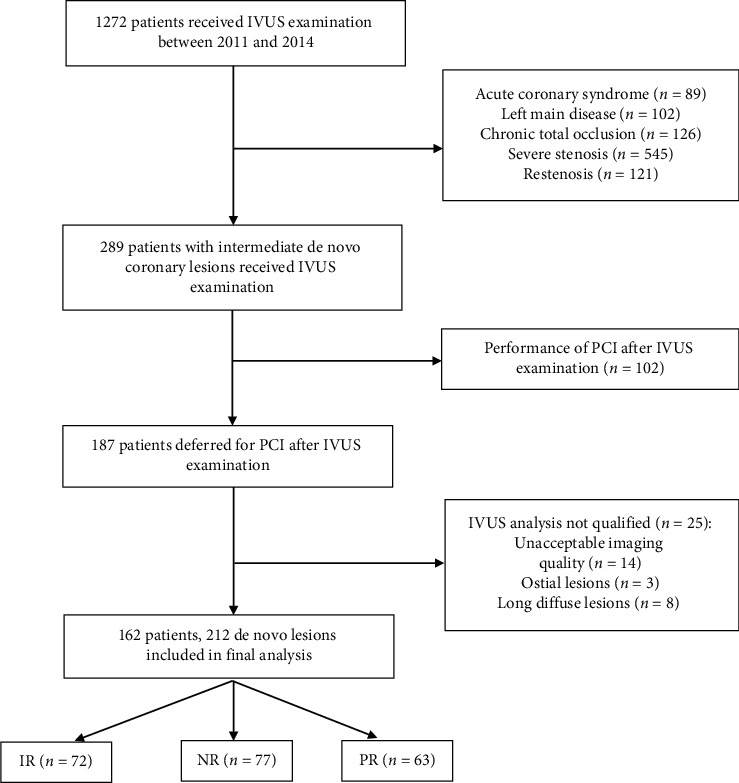
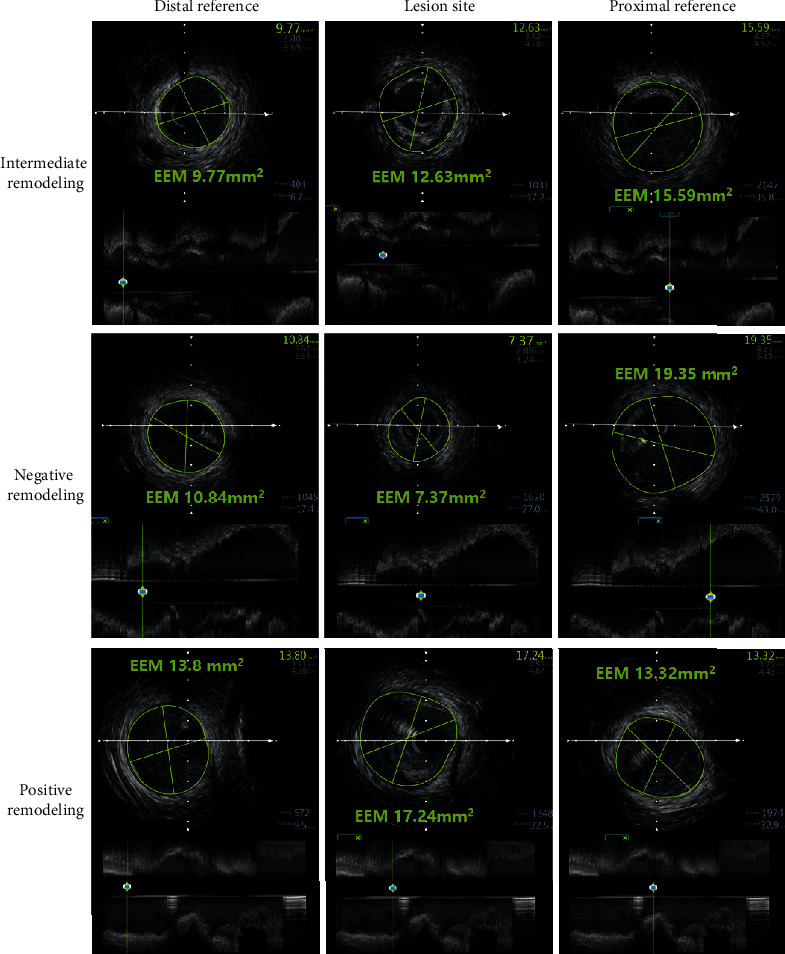
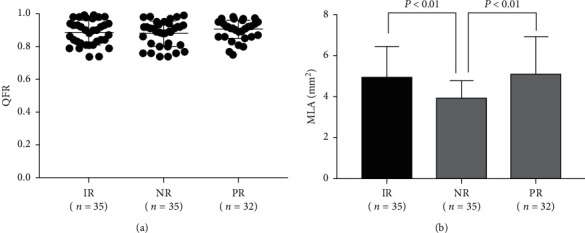
Methods: Arterial remodeling patterns were assessed in 212 deferred intermediate lesions from 162 patients after IVUS examination. Negative, intermediate, and positive remodeling was defined as a remodeling index of <0.88, 0.88∼1.0, and >1.0, respectively. The primary endpoint was the composite vessel-oriented clinical events, defined as the composition of target vessel-related cardiac death, target vessel-related myocardial infarction, and target vessel revascularization. Quantitative flow ratio was assessed for evaluating the functional significance of intermediate lesions.
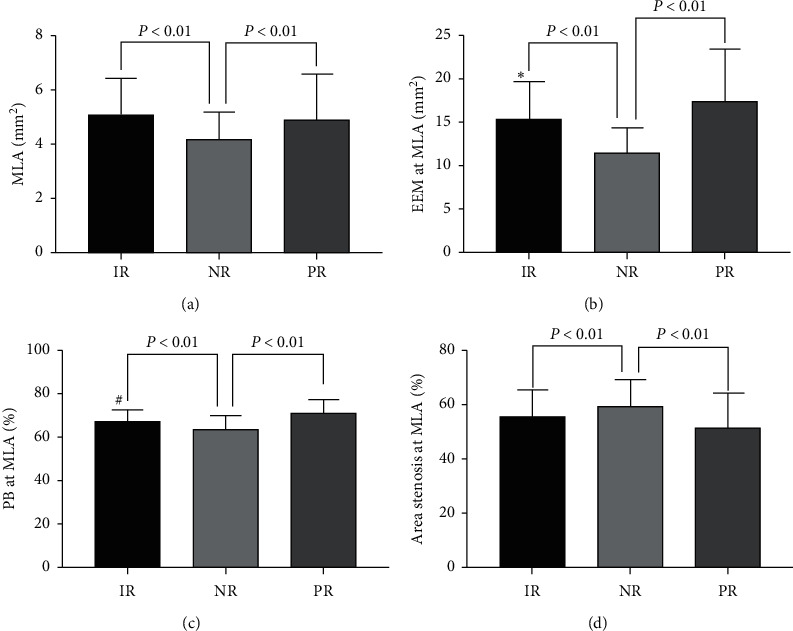
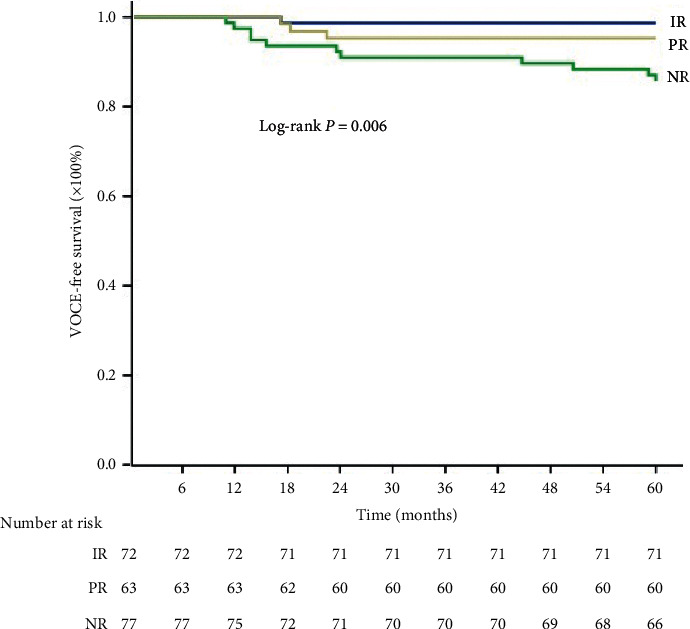
Results: 72 intermediate remodeling lesions were present in 66 patients, whereas 77 negative remodeling lesions were present in 71 patients, and 63 positive remodeling lesions were present in 55 patients. Negative remodeling lesions had the smallest minimum lumen area (4.16 ± 1.03 mm2 vs. 5.05 ± 1.39 mm2 vs. 4.85 ± 1.76 mm2; P < 0.01), smallest plaque burden (63.45 ± 6.13% vs. 66.12 ± 6.82% vs. 71.17 ± 6.45%; P < 0.01), and highest area stenosis rate (59.32% ± 10.15% vs. 54.61% ± 9.09% vs. 51.67% ± 12.96%; P < 0.01). No significant difference was found in terms of quantitative flow ratio among three groups. At 5 years follow-up, negative remodeling lesions had a higher rate of composite vessel-oriented clinical event (14.3%), compared to intermediate (1.4%, P=0.004) or positive remodeling lesions (4.8%, P=0.06). After adjusting for multiple covariates, negative remodeling remained an independent determinant for vessel-oriented clinical event (HR: 4.849, 95% CI 1.542-15.251, P=0.007).
Conclusion: IVUS-derived negative remodeling is associated with adverse long-term clinical outcome in stable patients with intermediate coronary artery stenosis.
Copyright © 2021 Liang Geng et al.
Conflict of interest statement
The authors declare that there are no conflicts of interest.
Figures
Similar articles
-
Prognostic Implications of Quantitative Flow Ratio and Plaque Characteristics in Intravascular Ultrasound-Guided Treatment Strategy.JACC Cardiovasc Interv. 2024 Feb 26;17(4):461-470. doi: 10.1016/j.jcin.2023.11.035. Epub 2024 Feb 7. JACC Cardiovasc Interv. 2024. PMID: 38340104
-
Impact of spotty calcification on long-term prediction of future revascularization: a prospective three-vessel intravascular ultrasound study.Heart Vessels. 2016 Jun;31(6):881-9. doi: 10.1007/s00380-015-0687-8. Epub 2015 May 12. Heart Vessels. 2016. PMID: 25964072
-
Long-term clinical outcomes in patients with untreated non-culprit intermediate coronary lesion and evaluation of predictors by using virtual histology-intravascular ultrasound; a prospective cohort study.BMC Cardiovasc Disord. 2019 Aug 5;19(1):187. doi: 10.1186/s12872-019-1173-5. BMC Cardiovasc Disord. 2019. PMID: 31382885 Free PMC article.
-
Influence of Anatomical and Clinical Characteristics on Long-Term Prognosis of FFR-Guided Deferred Coronary Lesions.JACC Cardiovasc Interv. 2020 Aug 24;13(16):1907-1916. doi: 10.1016/j.jcin.2020.05.040. JACC Cardiovasc Interv. 2020. PMID: 32819479
-
[New methods of coronary imaging II. Intracoronary ultrasonography in clinical practice].Ital Heart J Suppl. 2001 Jun;2(6):579-92. Ital Heart J Suppl. 2001. PMID: 11460831 Review. Italian.
Cited by
-
Whys and Wherefores of Coronary Arterial Positive Remodeling.Arterioscler Thromb Vasc Biol. 2024 Dec;44(12):2416-2427. doi: 10.1161/ATVBAHA.124.321504. Epub 2024 Oct 31. Arterioscler Thromb Vasc Biol. 2024. PMID: 39479766 Free PMC article. Review.
References
-
- Hahn J.-Y., Choi S.-H., Jeong J.-O., et al. Conservative versus aggressive treatment strategy with angiographic guidance alone in patients with intermediate coronary lesions: the SMART-CASE randomized, non-inferiority trial. International Journal of Cardiology. 2017;240:114–119. doi: 10.1016/j.ijcard.2017.03.075. - DOI - PubMed
-
- Kang J., Koo B.-K., Hu X., et al. Comparison of fractional flow reserve and intravascular ultrasound-guided intervention strategy for clinical Outcomes in patients with intermediate stenosis (FLAVOUR): rationale and design of a randomized clinical trial. American Heart Journal. 2018;199:7–12. doi: 10.1016/j.ahj.2017.11.001. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
