

Development and Validation of a Nomogram Based on Noninvasive Liver Reserve and Fibrosis (PALBI and FIB-4) Model to Predict Posthepatectomy Liver Failure Grade B-C in Patients with Hepatocellular Carcinoma
- PMID: 34221013
- PMCID: PMC8221058
- DOI: 10.1155/2021/6665267
Development and Validation of a Nomogram Based on Noninvasive Liver Reserve and Fibrosis (PALBI and FIB-4) Model to Predict Posthepatectomy Liver Failure Grade B-C in Patients with Hepatocellular Carcinoma
Abstract
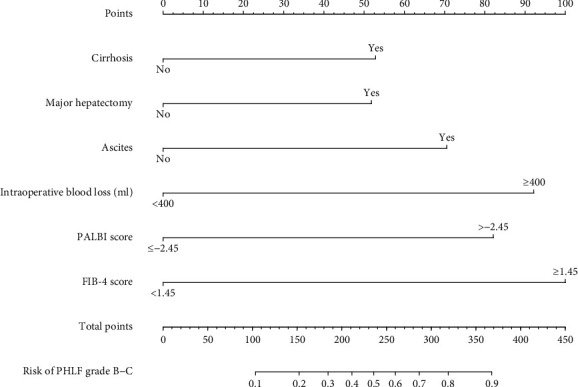
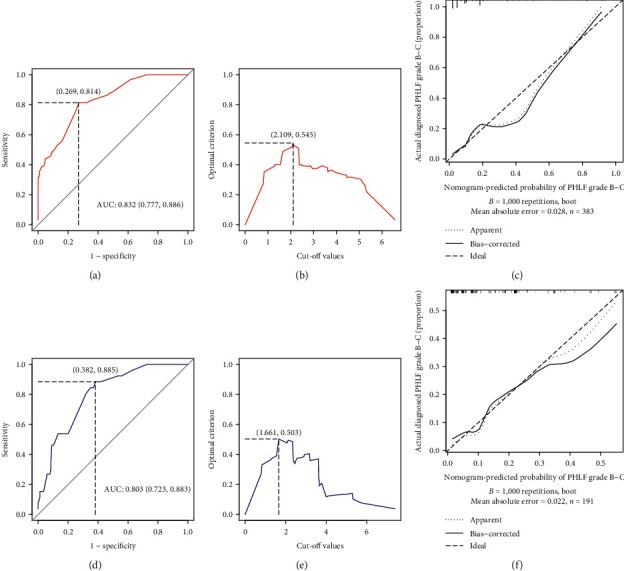
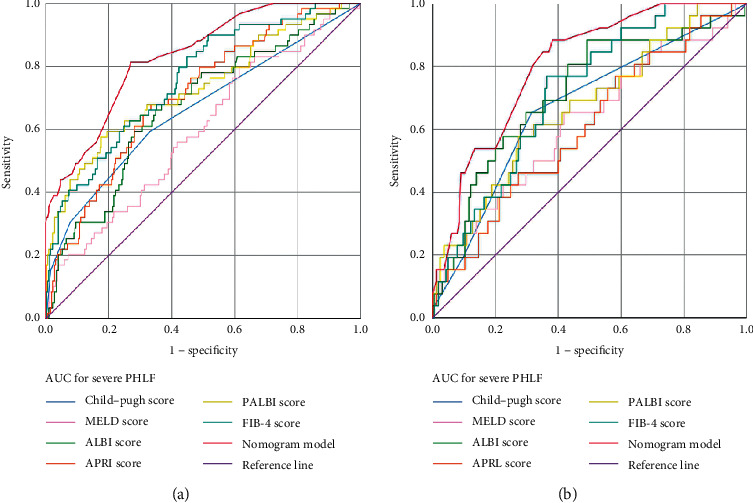
Hepatectomy is currently one of the most effective treatments for hepatocellular carcinoma (HCC). However, postoperative liver failure (PHLF) is a serious complication and the leading cause of mortality in patients with HCC after hepatectomy. This study attempted to develop a novel nomogram based on noninvasive liver reserve and fibrosis models, platelet-albumin-bilirubin grade (PALBI) and fibrosis-4 index (FIB-4), able to predict PHLF grade B-C. This was a single-centre retrospective study of 574 patients with HCC undergoing hepatectomy between 2014 and 2018. The independent risk factors of PHLF were screened using univariate and multivariate logistic regression analyses. Multivariate logistic regression was performed using the training set, and the nomogram was developed and visualised. The utility of the model was evaluated in a validation set using the receiver operating characteristic (ROC) curve. A total of 574 HCC patients were included (383 in the training set and 191 for the validation set) and included PHLF grade B-C complications of 14.8, 15.4, and 13.6%, respectively. Overall, cirrhosis (P < 0.026, OR = 2.296, 95% confidence interval (CI) 1.1.02-4.786), major hepatectomy (P=0.031, OR = 2.211, 95% CI 1.077-4.542), ascites (P=0.014, OR = 3.588, 95% 1.299-9.913), intraoperative blood loss (P < 0.001, OR = 4.683, 95% CI 2.281-9.616), PALBI score >-2.53 (, OR = 3.609, 95% CI 1.486-8.764), and FIB-4 score ≥1.45 (P < 0.001, OR = 5.267, 95% CI 2.077-13.351) were identified as independent risk factors associated with PHLF grade B-C in the training set. The areas under the ROC curves for the nomogram model in predicting PHLF grade B-C were significant for both the training and validation sets (0.832 vs 0.803). The proposed nomogram predicted PHLF grade B-C among patients with HCC with a better prognostic accuracy than other currently available fibrosis and noninvasive liver reserve models.
Copyright © 2021 Wenhui Zhong et al.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures
References
-
- Kim Y. S., Shin S. W. Hepatocellular carcinoma. New England Journal of Medicine. 2019;381(1):p. e2. - PubMed
LinkOut - more resources
Full Text Sources
