

Barium Defecating Proctography and Dynamic Magnetic Resonance Proctography: Their Role and Patient's Perception
- PMID: 34221640
- PMCID: PMC8247951
- DOI: 10.25259/JCIS_56_2021
Barium Defecating Proctography and Dynamic Magnetic Resonance Proctography: Their Role and Patient's Perception
Abstract
Objectives: The objectives of the study were to compare the imaging findings and patient's perception of barium defecating proctography and dynamic magnetic resonance (MR) proctography in patients with pelvic floor disorders.
Material and methods: This is a prospective study conducted on patients with pelvic floor disorders who consented to undergo both barium proctography and dynamic MR proctography. Imaging findings of both the procedures were compared. Inter-observer agreement (IOA) for key imaging features was assessed. Patient's perception of these procedures was assessed using a short questionnaire and a visual analog scale.
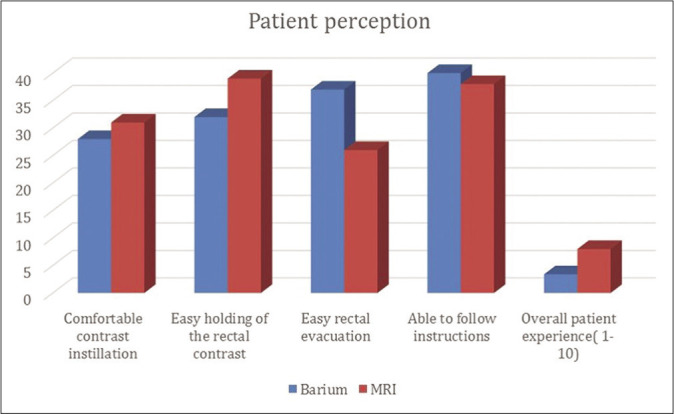
Results: Forty patients (M: F =19:21) with a mean age of 43.65 years and range of 21-75 years were included for final analysis. Mean patient experience score was significantly better for MR imaging (MRI) (p < 0.001). However, patients perceived significantly higher difficulty in rectal evacuation during MRI studies (p = 0.003). While significantly higher number of rectoceles (p = 0.014) were diagnosed on MRI, a greater number of pelvic floor descent (p = 0.02) and intra-rectal intussusception (p = 0.011) were diagnosed on barium proctography. The IOA for barium proctography was substantial for identifying rectoceles, rectal prolapse and for determining M line, p < 0.001. There was excellent IOA for MRI interpretation of cystoceles, peritoneoceles, and uterine prolapse and substantial to excellent IOA for determining anal canal length and anorectal angle, p < 0.001. The mean study time for the barium and MRI study was 12 minutes and 15 minutes, respectively.
Conclusion: Barium proctography was more sensitive than MRI for detecting pelvic floor descent and intrarectal intussusception. Although patients perceived better rectal emptying with barium proctography, the overall patient experience was better for dynamic MRI proctography.
Keywords: Accuracy; Barium proctography; Diagnosis; Imaging; Magnetic resonance proctography; Pelvic floor.
© 2021 Published by Scientific Scholar on behalf of Journal of Clinical Imaging Science.
Conflict of interest statement
There are no conflicts of interest.
Figures









Similar articles
-
Barium proctography vs magnetic resonance proctography for pelvic floor disorders: a comparative study.Colorectal Dis. 2012 Oct;14(10):1224-30. doi: 10.1111/j.1463-1318.2012.02945.x. Colorectal Dis. 2012. PMID: 22251617 Clinical Trial.
-
Dynamic transperineal ultrasound in the diagnosis of pelvic floor disorders: pilot study.Dis Colon Rectum. 2002 Feb;45(2):239-45; discussion 245-8. doi: 10.1007/s10350-004-6155-7. Dis Colon Rectum. 2002. PMID: 11852339
-
Integrated total pelvic floor ultrasound in pelvic floor defaecatory dysfunction.Colorectal Dis. 2017 Jan;19(1):O54-O65. doi: 10.1111/codi.13568. Colorectal Dis. 2017. PMID: 27886434
-
Defecating proctography: A pictorial essay.Radiography (Lond). 2022 Aug;28(3):628-633. doi: 10.1016/j.radi.2022.04.012. Epub 2022 May 12. Radiography (Lond). 2022. PMID: 35569315 Review.
-
Evacuation proctography (defecography): an aid to the investigation of pelvic floor disorders.Obstet Gynecol. 1994 Feb;83(2):307-14. Obstet Gynecol. 1994. PMID: 8290201 Review.
Cited by
-
Comparison of Dynamic Magnetic Resonance Defecography With Clinical Examination in Diagnosing Pelvic Floor Dysfunction: An Observational Study.Cureus. 2023 Dec 31;15(12):e51378. doi: 10.7759/cureus.51378. eCollection 2023 Dec. Cureus. 2023. PMID: 38292993 Free PMC article.
-
Magnetic resonance defecography assessment of obstructed defecation syndrome in patients with chronic constipation in a tertiary care hospital.World J Radiol. 2025 May 28;17(5):106102. doi: 10.4329/wjr.v17.i5.106102. World J Radiol. 2025. PMID: 40503482 Free PMC article.
-
Ventral mesh rectopexy. Does a descending perineum impact functional results and quality of life?Langenbecks Arch Surg. 2024 Jan 19;409(1):44. doi: 10.1007/s00423-024-03236-9. Langenbecks Arch Surg. 2024. PMID: 38240901
References
LinkOut - more resources
Full Text Sources