

Fluidic Considerations of Measuring Intracranial Pressure Using an Open External Ventricular Drain
- PMID: 34221772
- PMCID: PMC8239198
- DOI: 10.7759/cureus.15324
Fluidic Considerations of Measuring Intracranial Pressure Using an Open External Ventricular Drain
Abstract
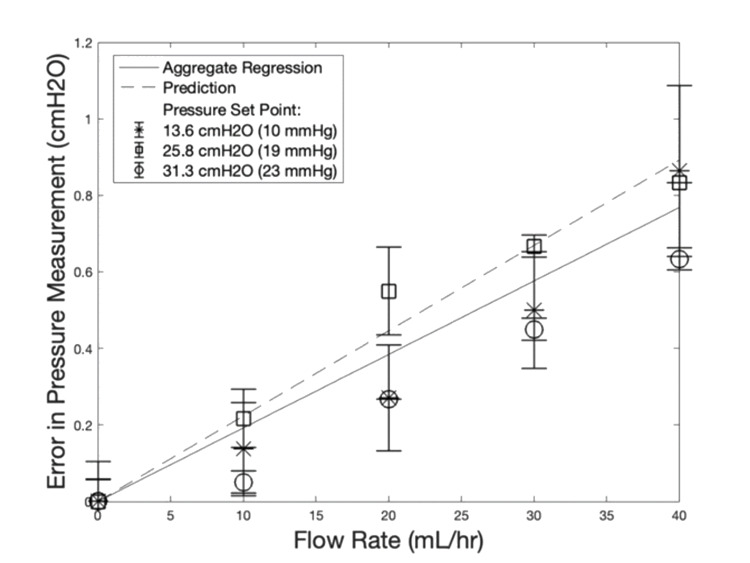
Measurement of intracranial pressure (ICP) during cerebrospinal fluid (CSF) drainage with an external ventricular drain (EVD) typically requires stopping the flow during measurement. However, there may be benefits to simultaneous ICP measurement and CSF drainage. Several studies have evaluated whether accurate ICP measurements can be obtained while the EVD is open. They report differing outcomes when it comes to error, and hypothesize several sources of error. This study presents an investigation into the fluidic sources of error for ICP measurement with concurrent drainage in an EVD. Our experiments and analytical model both show that the error in pressure measurement increases linearly with flow rate and is not clinically significant, regardless of drip chamber height. At physiologically relevant flow rates (40 mL/hr) and ICP set points (13.6 - 31.3 cmH2O or 10 - 23 mmHg), our model predicts an underestimation of 0.767 cmH2O (0.56 mmHg) with no observed data point showing error greater than 1.09 cmH2O (0.8 mmHg) in our experiment. We extrapolate our model to predict a realistic worst-case clinical scenario where we expect to see a mean maximum error of 1.06 cmH2O (0.78 mmHg) arising from fluidic effects within the drainage system for the most resistive catheter. Compared to other sources of error in current ICP monitoring, error in pressure measurement due to drainage flow is small and does not prohibit clinical use. However, other effects such as ventricular collapse or catheter obstruction could affect ICP measurement under continuous drainage and are not investigated in this study.
Keywords: bioengineering; catheter; cerebrospinal fluid; continuous measurement; external ventricular drain; intracranial hypertension; neuro-monitoring; neuro-surgery; neurology and critical care; traumatic brain injury.
Copyright © 2021, Beidler et al.
Conflict of interest statement
BL and SB are Founders of Aqueduct Neurosciences, Inc that was founded to develop CSF drainage technologies, and they are inventors on patents on CSF drainage technologies.
Figures


References
-
- Javed K, Reddy V, Lui F. StatPearls [Internet] Treasure Island: StatPearls Publishing; 2021 Jan-. Neuroanatomy, choroid plexus [updated 2020 Jul 31] - PubMed
-
- Telano LN, Baker S. StatPearls [Internet} Treasure Island: StatPearls Publishing; 2021 Jan-. Physiology, cerebral spinal fluid [updated 2020 Jul 14] - PubMed
-
- Guidelines for the management of severe traumatic brain injury, fourth edition. Carney N, Totten AM, O'Reilly C, et al. Neurosurgery. 2017;80:6–15. - PubMed
-
- Duet EDMS System - Indications, Safety & Warnings | Medtronic. [Feb;2021 ];https://www.medtronic.com/us-en/healthcare-professionals/products/neurol... 2021
-
- Critical care management of increased intracranial pressure. Mayer SA, Chong JY. J Intensive Care Med. 2002;17:55–67.
LinkOut - more resources
Full Text Sources
Other Literature Sources