

Out-of-Hospital Cervical Ripening With a Synthetic Hygroscopic Cervical Dilator May Reduce Hospital Costs and Cesarean Sections in the United States-A Cost-Consequence Analysis
- PMID: 34222185
- PMCID: PMC8249762
- DOI: 10.3389/fpubh.2021.689115
Out-of-Hospital Cervical Ripening With a Synthetic Hygroscopic Cervical Dilator May Reduce Hospital Costs and Cesarean Sections in the United States-A Cost-Consequence Analysis
Abstract
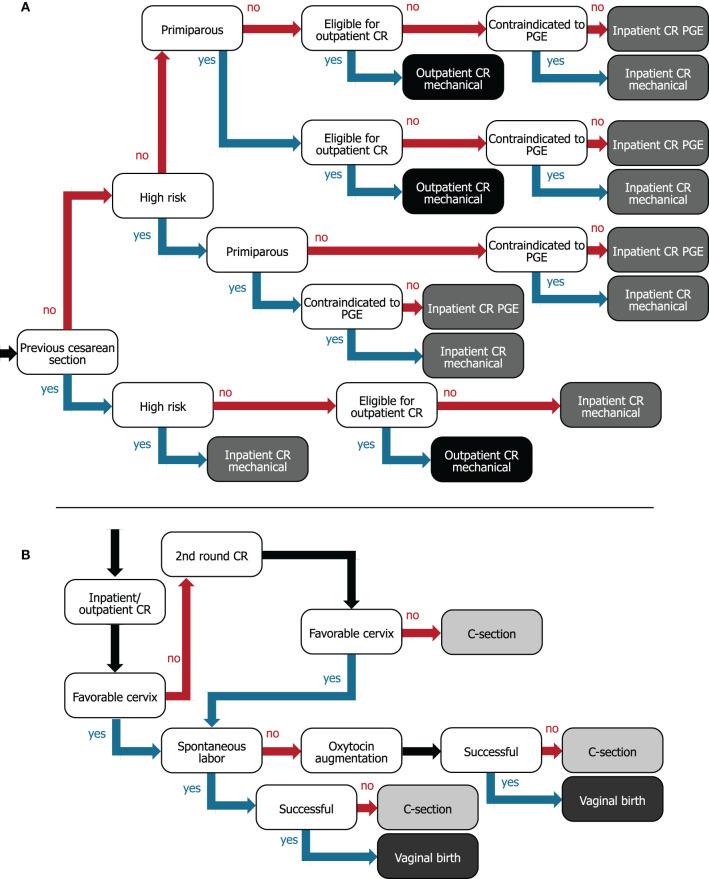
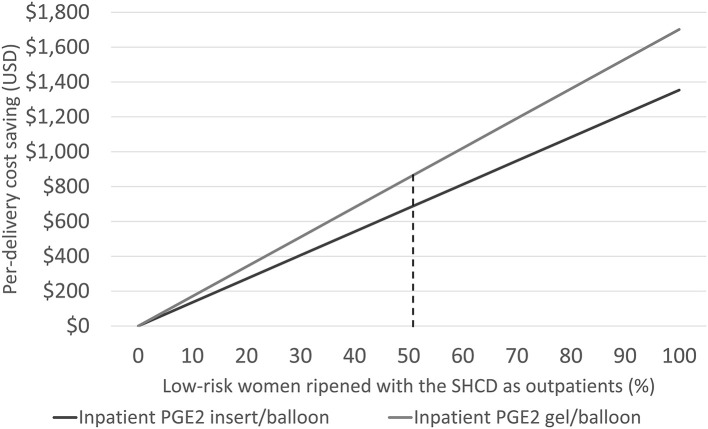
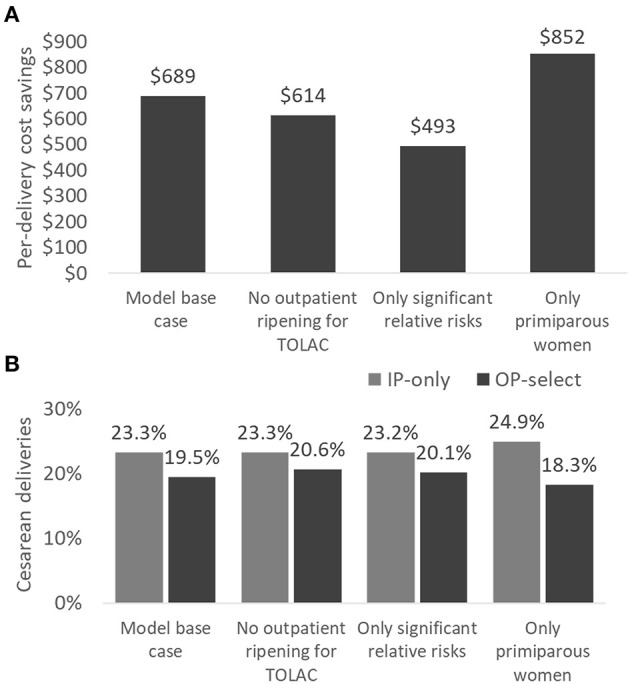
Objective: Out-of-hospital (outpatient) cervical ripening prior to induction of labor (IOL) is discussed for its potential to decrease the burden on hospital resources. We assessed the cost and clinical outcomes of adopting an outpatient strategy with a synthetic hygroscopic cervical dilator, which is indicated for use in preinduction cervical ripening. Methods: We developed a cost-consequence model from the hospital perspective with a time period from IOL to post-delivery discharge. A hypothetical cohort of women to undergo IOL at term with an unfavorable cervix (all risk levels) were assessed. As the standard of care (referred to as IP-only) all women were ripened as inpatients using the vaginal PGE2 insert or the single-balloon catheter. In the comparison (OP-select), 50.9% of low-risk women (41.4% of the study population) received outpatient cervical ripening using a synthetic hygroscopic cervical dilator and the remaining women were ripened as inpatients as in the standard of care. Model inputs were sourced from a structured literature review of peer-reviewed articles in PubMed. Testing of 2,000 feasible scenarios (probabilistic multivariate sensitivity analysis) ascertained the robustness of results. Outcomes are reported as the average over all women assessed, comparing OP-select to IP-only. Results: Implementing OP-select resulted in hospital savings of US$689 per delivery, with women spending 1.48 h less time in the labor and delivery unit and 0.91 h less in the postpartum recovery unit. The cesarean-section rate was decreased by 3.78 percentage points (23.28% decreased to 19.50%). In sensitivity testing, hospital costs and cesarean-section rate were reduced in 91% of all instances. Conclusion: Our model analysis projects that outpatient cervical ripening has the potential to reduce hospital costs, hospital stay, and the cesarean section rate. It may potentially allow for better infection-prevention control during the ongoing COVID-19 pandemic and to free up resources such that more women might be offered elective IOL at 39 weeks.
Keywords: cervical ripening; cesarean section; cost-consequence analysis; health economics; induction of labor; mechanical dilator; outpatient; prostaglandins.
Copyright © 2021 Saunders, Saunders, Wong and Saad.
Conflict of interest statement
SS was an employee and RS was the owner of Coreva Scientific GmbH & Co KG, which received consultancy fees for performing, analyzing, and communicating the work presented here. TW was an employee of Medicem Inc., the US agent and initial importer of Dilapan-S® and company funding this research. AS was an expert consultant and part of the advisory board for the sponsor. This study was funded by Medicem Inc. (USA). Medicem, Inc. contracted Coreva Scientific to perform this work and provided background details for the conceptual design of the analysis and reviewed the model and manuscript.
Figures
Similar articles
-
Moving preinduction cervical ripening to a lower acuity inpatient setting using the synthetic hygroscopic cervical dilator: a cost-consequence analysis for the United States.J Med Econ. 2022 Jan-Dec;25(1):1185-1198. doi: 10.1080/13696998.2022.2136854. J Med Econ. 2022. PMID: 36274625
-
Cervical ripening as an outpatient procedure in the pandemic - minimizing the inpatient days and lowering the socioeconomic costs.J Perinat Med. 2022 Aug 9;50(9):1180-1188. doi: 10.1515/jpm-2022-0196. Print 2022 Nov 25. J Perinat Med. 2022. PMID: 35942570
-
Randomized control trial comparing hygroscopic cervical dilators to cervical ripening balloon for outpatient cervical ripening.Am J Obstet Gynecol MFM. 2024 Apr;6(4):101318. doi: 10.1016/j.ajogmf.2024.101318. Epub 2024 Feb 28. Am J Obstet Gynecol MFM. 2024. PMID: 38417552 Clinical Trial.
-
Preinduction cervical ripening: basis and methods of current practice.Obstet Gynecol Surv. 2002 Oct;57(10):683-92. doi: 10.1097/00006254-200210000-00022. Obstet Gynecol Surv. 2002. PMID: 12368596 Review.
-
Outpatient Cervical Ripening with Balloon Catheters: A Systematic Review and Meta-analysis.Obstet Gynecol. 2022 Feb 1;139(2):255-268. doi: 10.1097/AOG.0000000000004644. Obstet Gynecol. 2022. PMID: 34991144
Cited by
-
Comparison of outpatient with inpatient mifepristone usage for cervical ripening: A randomised controlled trial.Eur J Obstet Gynecol Reprod Biol X. 2023 May 16;18:100198. doi: 10.1016/j.eurox.2023.100198. eCollection 2023 Jun. Eur J Obstet Gynecol Reprod Biol X. 2023. PMID: 37234794 Free PMC article.
-
Predictive Factors for the Success of Vaginal Dinoprostone for the Induction of Labour.Int J Womens Health. 2024 Jun 13;16:1093-1101. doi: 10.2147/IJWH.S461094. eCollection 2024. Int J Womens Health. 2024. PMID: 38887592 Free PMC article.
-
Synthetic Osmotic Dilators for Pre-Induction Cervical Ripening - an Evidence-Based Review.Geburtshilfe Frauenheilkd. 2023 Jul 7;83(12):1491-1499. doi: 10.1055/a-2103-8329. eCollection 2023 Dec. Geburtshilfe Frauenheilkd. 2023. PMID: 38046527 Free PMC article.
References
-
- Martin JA, Hamilton BE, Sutton PD, Ventura SJ, Menacker F, Kirmeyer S, et al. . National vital statistics reports births : final data for 2018. Natl Vital Statisctics Rep. (2019) 68:1–47. Available online at: https://www.cdc.gov/nchs/data/nvsr/nvsr68/nvsr68_13-508.pdf
-
- Clinical Guidance for Integration of the Findings of The ARRIVE Trial: Labor Induction Versus Expectant Management in Low-Risk Nulliparous Women | ACOG [Internet]. Available online at: https://www.acog.org/clinical/clinical-guidance/practice-advisory/articl... (accessed November 27, 2020).
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous