Quality control of radiomic features using 3D-printed CT phantoms
- PMID: 34222557
- PMCID: PMC8240751
- DOI: 10.1117/1.JMI.8.3.033505
Quality control of radiomic features using 3D-printed CT phantoms
Abstract
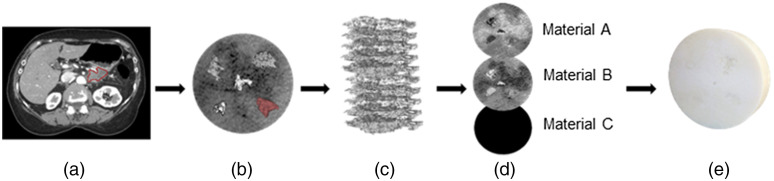
Purpose: The lack of standardization in quantitative radiomic measures of tumors seen on computed tomography (CT) scans is generally recognized as an unresolved issue. To develop reliable clinical applications, radiomics must be robust across different CT scan modes, protocols, software, and systems. We demonstrate how custom-designed phantoms, imprinted with human-derived patterns, can provide a straightforward approach to validating longitudinally stable radiomic signature values in a clinical setting. Approach: Described herein is a prototype process to design an anatomically informed 3D-printed radiomic phantom. We used a multimaterial, ultra-high-resolution 3D printer with voxel printing capabilities. Multiple tissue regions of interest (ROIs), from four pancreas tumors, one lung tumor, and a liver background, were extracted from digital imaging and communication in medicine (DICOM) CT exam files and were merged together to develop a multipurpose, circular radiomic phantom (18 cm diameter and 4 cm width). The phantom was scanned 30 times using standard clinical CT protocols to test repeatability. Features that have been found to be prognostic for various diseases were then investigated for their repeatability and reproducibility across different CT scan modes. Results: The structural similarity index between the segment used from the patients' DICOM image and the phantom CT scan was 0.71. The coefficient variation for all assessed radiomic features was across 30 repeat scans of the phantom. The percent deviation (pDV) from the baseline value, which was the mean feature value determined from repeat scans, increased with the application of the lung convolution kernel, changes to the voxel size, and increases in the image noise. Gray level co-occurrence features, contrast, dissimilarity, and entropy were particularly affected by different scan modes, presenting with . Conclusions: Previously discovered prognostic and popular radiomic features are variable in practice and need to be interpreted with caution or excluded from clinical implementation. Voxel-based 3D printing can reproduce tissue morphology seen on CT exams. We believe that this is a flexible, yet practical, way to design custom phantoms to validate and compare radiomic metrics longitudinally, over time, and across systems.
Keywords: additive manufacturing; computed tomography; quantitative imaging; radiomics.
© 2021 The Authors.
Figures