

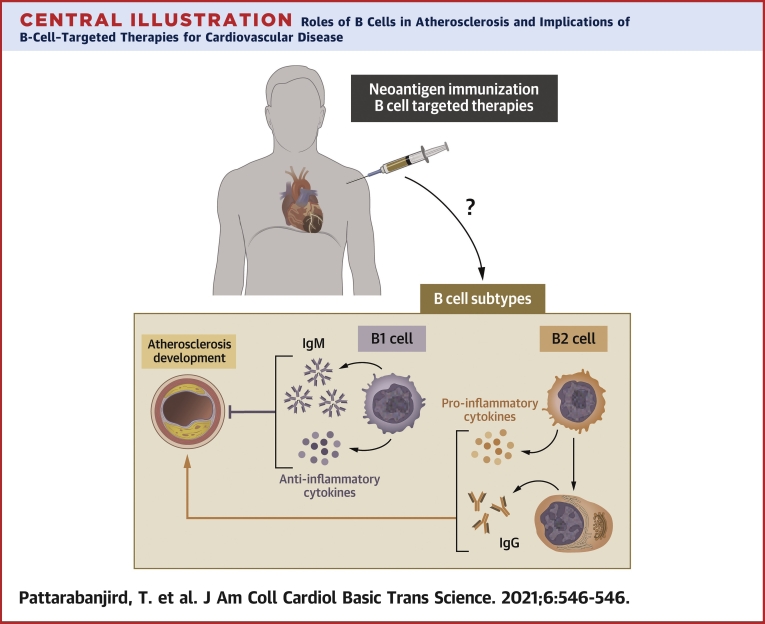
B Cells in Atherosclerosis: Mechanisms and Potential Clinical Applications
- PMID: 34222726
- PMCID: PMC8246059
- DOI: 10.1016/j.jacbts.2021.01.006
B Cells in Atherosclerosis: Mechanisms and Potential Clinical Applications
Abstract
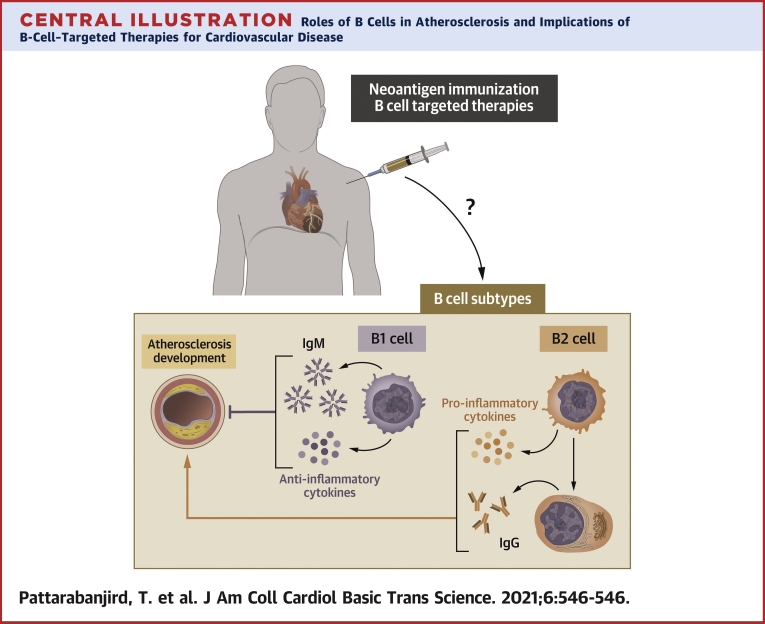
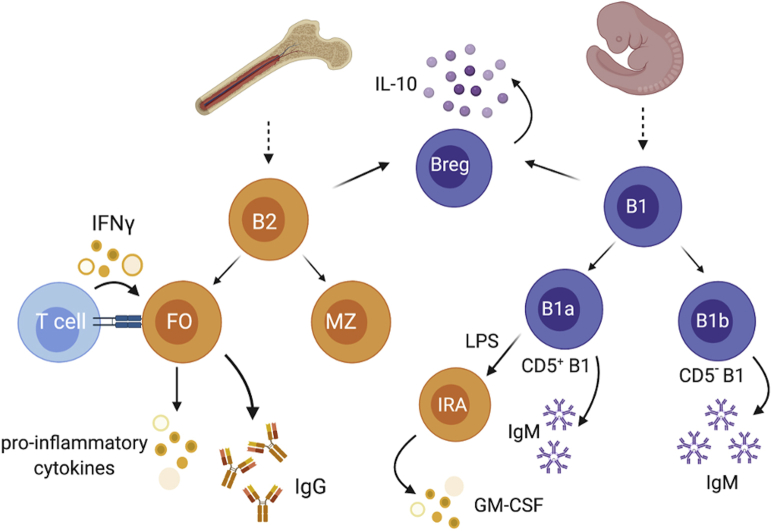
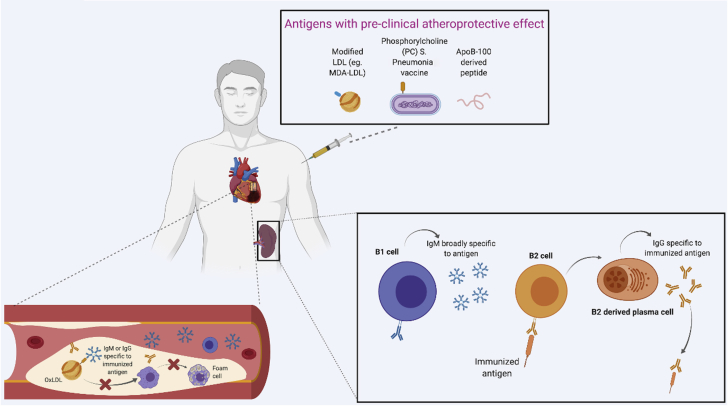
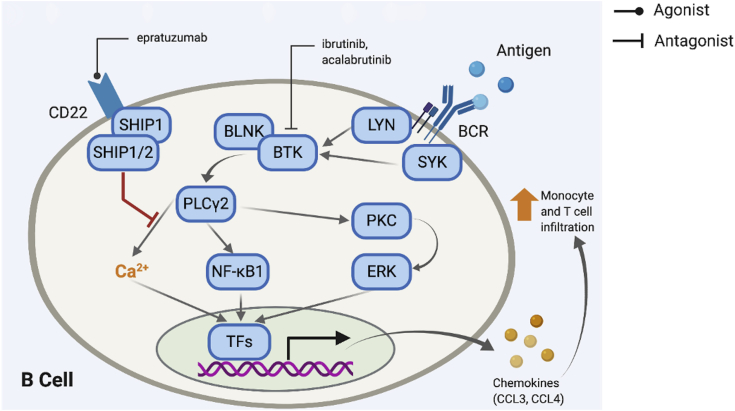
Because atherosclerotic cardiovascular disease is a leading cause of death worldwide, understanding inflammatory processes underpinning its pathology is critical. B cells have been implicated as a key immune cell type in regulating atherosclerosis. B-cell effects, mediated by antibodies and cytokines, are subset specific. In this review, we focus on elaborating mechanisms underlying subtype-specific roles of B cells in atherosclerosis and discuss available human data implicating B cells in atherosclerosis. We further discuss potential B cell-linked therapeutic approaches, including immunization and B cell-targeted biologics. Given recent evidence strongly supporting a role for B cells in human atherosclerosis and the expansion of immunomodulatory agents that affect B-cell biology in clinical use and clinical trials for other disorders, it is important that the cardiovascular field be cognizant of potential beneficial or untoward effects of modulating B-cell activity on atherosclerosis.
Keywords: APRIL, A proliferation−inducing ligand; ApoE, apolipoprotein E; B-cell; BAFF, B-cell–activating factor; BAFFR, B-cell–activating factor receptor; BCMA, B-cell maturation antigen; BCR, B-cell receptor; Breg, regulatory B cell; CAD, coronary artery disease; CTLA4, cytotoxic T-lymphocyte–associated protein 4; CVD, cardiovascular disease; CXCR4, C-X-C motif chemokine receptor 4; GC, germinal center; GITR, glucocorticoid-induced tumor necrosis factor receptor–related protein; GITRL, glucocorticoid-induced tumor necrosis factor receptor–related protein ligand; GM-CSF, granulocyte-macrophage colony–stimulating factor; ICI, immune checkpoint inhibitor; IFN, interferon; IL, interleukin; IVUS, intravascular ultrasound; LDL, low-density lipoprotein; LDLR, low-density lipoprotein receptor; MDA-LDL, malondialdehyde-modified low-density lipoprotein; MI, myocardial infarction; OSE, oxidation-specific epitope; OxLDL, oxidized low-density lipoprotein; PC, phosphorylcholine; PD-1, programmed cell death protein 1; PD-L2, programmed death ligand 2; PDL1, programmed death ligand 1; RA, rheumatoid arthritis; SLE, systemic lupus erythematosus; TACI, transmembrane activator and CAML interactor; TNF, tumor necrosis factor; Treg, regulatory T cell; atherosclerosis; immunoglobulins; mAb, monoclonal antibody.
© 2021 The Authors.
Conflict of interest statement
The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Similar articles
-
Biological drug and drug delivery-mediated immunotherapy.Acta Pharm Sin B. 2021 Apr;11(4):941-960. doi: 10.1016/j.apsb.2020.12.018. Epub 2020 Dec 31. Acta Pharm Sin B. 2021. PMID: 33996408 Free PMC article. Review.
-
Re-thinking the functions of IgA(+) plasma cells.Gut Microbes. 2014;5(5):652-62. doi: 10.4161/19490976.2014.969977. Gut Microbes. 2014. PMID: 25483334 Free PMC article. Review.
-
B Cell-Activating Factor Neutralization Aggravates Atherosclerosis.Circulation. 2018 Nov 13;138(20):2263-2273. doi: 10.1161/CIRCULATIONAHA.117.032790. Circulation. 2018. PMID: 29858401 Free PMC article.
-
BAFF-R and TACI expression on CD3+ T cells: Interplay among BAFF, APRIL and T helper cytokines profile in systemic lupus erythematosus.Cytokine. 2019 Feb;114:115-127. doi: 10.1016/j.cyto.2018.11.008. Epub 2018 Nov 19. Cytokine. 2019. PMID: 30467093
-
Effects of BAFF Neutralization on Atherosclerosis Associated With Systemic Lupus Erythematosus.Arthritis Rheumatol. 2021 Feb;73(2):255-264. doi: 10.1002/art.41485. Epub 2020 Dec 15. Arthritis Rheumatol. 2021. PMID: 32783382
Cited by
-
Single-cell profiling of CD11c+ B cells in atherosclerosis.Front Immunol. 2024 Jan 8;14:1296668. doi: 10.3389/fimmu.2023.1296668. eCollection 2023. Front Immunol. 2024. PMID: 38259450 Free PMC article.
-
Editorial: New insights of immune cells in cardiovascular and metabolic disorders.Front Immunol. 2023 Sep 28;14:1282078. doi: 10.3389/fimmu.2023.1282078. eCollection 2023. Front Immunol. 2023. PMID: 37841242 Free PMC article. No abstract available.
-
The role of immunoglobins in atherosclerosis development; friends or foe?Mol Cell Biochem. 2025 May;480(5):2737-2747. doi: 10.1007/s11010-024-05158-y. Epub 2024 Nov 27. Mol Cell Biochem. 2025. PMID: 39592554 Review.
-
Genetic association with autoimmune diseases identifies molecular mechanisms of coronary artery disease.iScience. 2024 Aug 13;27(9):110715. doi: 10.1016/j.isci.2024.110715. eCollection 2024 Sep 20. iScience. 2024. PMID: 39262791 Free PMC article.
-
Causal relationship between immune cells and risk of myocardial infarction: evidence from a Mendelian randomization study.Front Cardiovasc Med. 2024 Aug 27;11:1416112. doi: 10.3389/fcvm.2024.1416112. eCollection 2024. Front Cardiovasc Med. 2024. PMID: 39257847 Free PMC article.
References
-
- Virani S.S., Alonso A., Benjamin E.J. Heart disease and stroke statistics—2020 update: a report from the American Heart Association. Circulation. 2020;141:e139–e596. - PubMed
-
- Ross R., Glomset J.A. The pathogenesis of atherosclerosis. N Engl J Med. 1976;295:369–377. - PubMed
-
- Schwartz C.J., Mitchell J.R. Cellular infiltration of the human arterial adventitia associated with atheromatous plaques. Circulation. 1962;26:73–78. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
