

Evaluating cognitive profiles of patients undergoing clinical amyloid-PET imaging
- PMID: 34222867
- PMCID: PMC8244634
- DOI: 10.1093/braincomms/fcab035
Evaluating cognitive profiles of patients undergoing clinical amyloid-PET imaging
Abstract
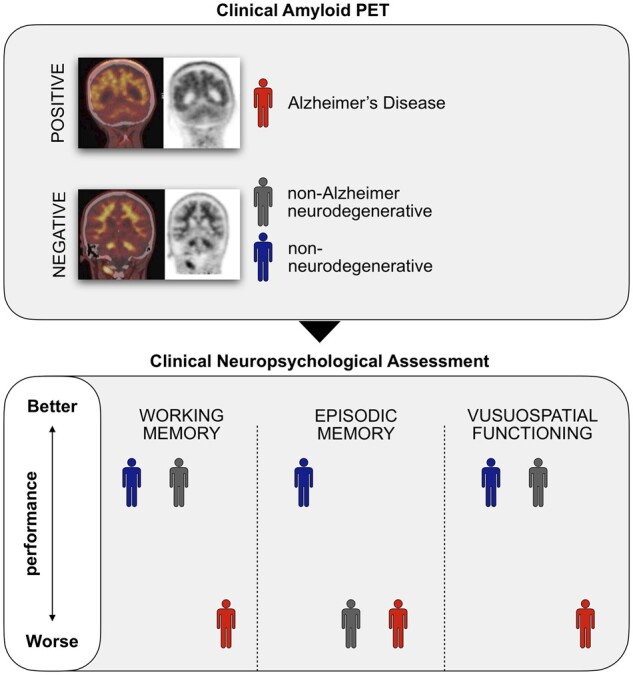
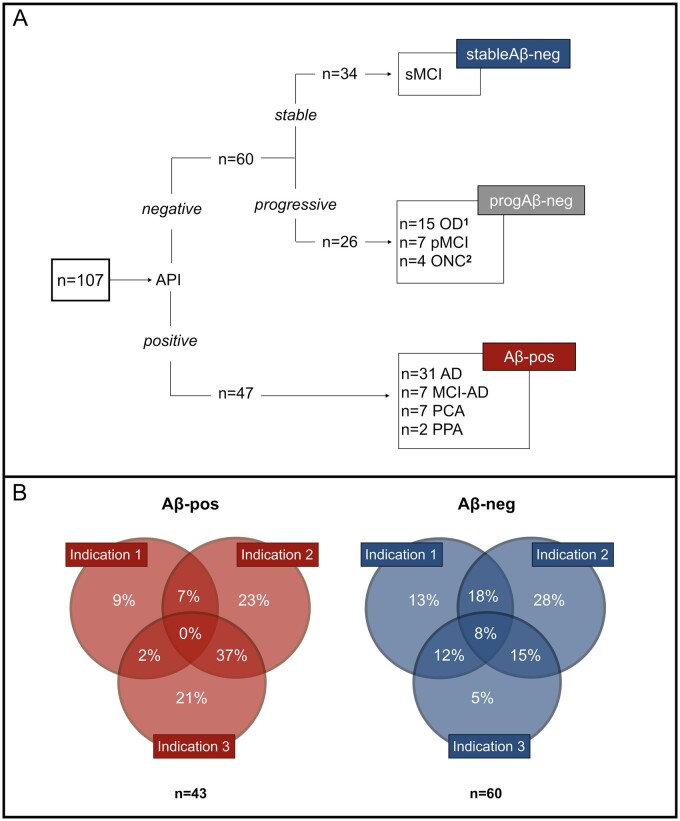
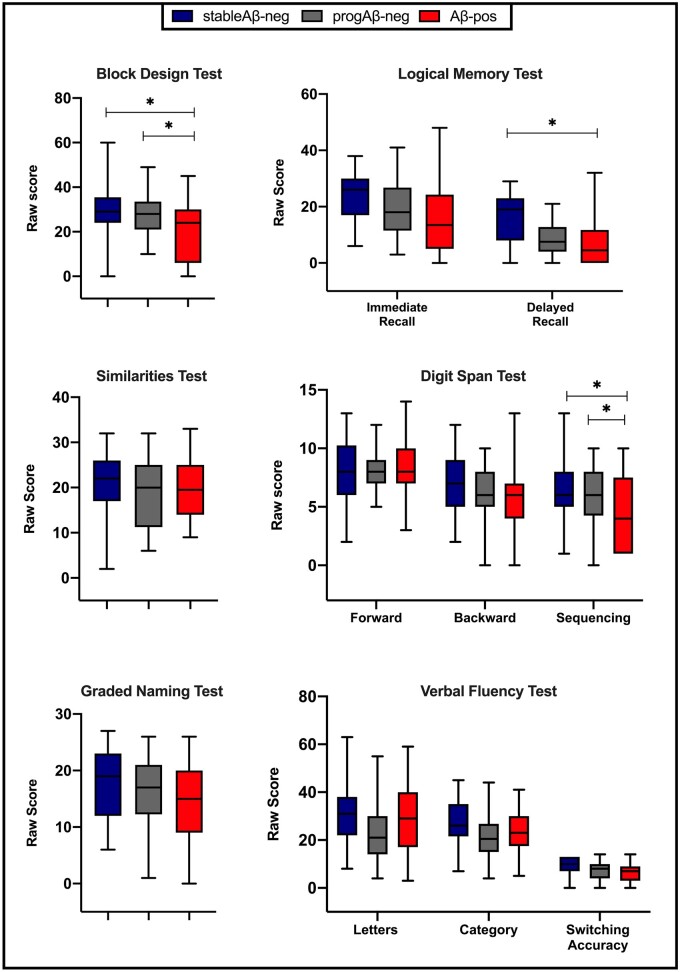
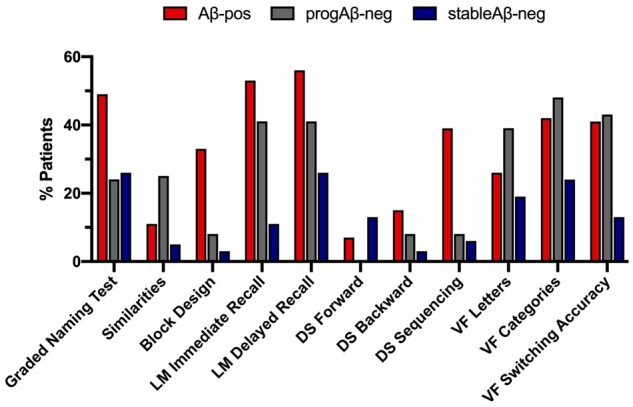
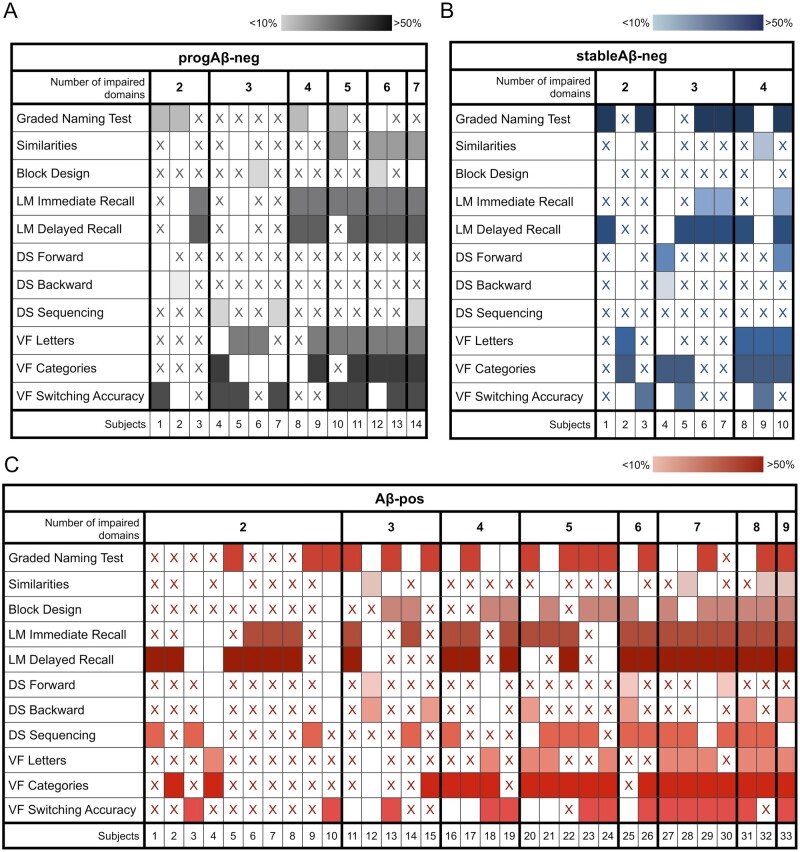
Episodic memory impairment and brain amyloid-beta are two of the main hallmarks of Alzheimer's Disease. In the clinical setting, these are often evaluated through neuropsychological testing and amyloid PET imaging, respectively. The use of amyloid PET in clinical practice is only indicated in patients with substantial diagnostic uncertainty due to atypical clinical presentation, multiple comorbidities and/or early age of onset. The relationship between amyloid-beta and cognition has been previously investigated, but no study has examined how neuropsychological features relate to the presence of amyloid pathology in the clinical population that meets the appropriate use criteria for amyloid PET imaging. In this study, we evaluated a clinical cohort of patients (n = 107) who presented at the Imperial Memory Clinic and were referred for clinical amyloid PET and neuropsychological assessment as part of their diagnostic workup. We compared the cognitive performance of amyloid-positive patients (Aβ-pos, n = 47) with that of stable amyloid-negative (stableAβ-neg, n = 26) and progressive amyloid-negative (progAβ-neg, n = 34) patients. The amyloid-positive group performed significantly worse than both amyloid-negative groups in the visuospatial and working memory domains. Episodic memory performance, however, effectively differentiated the amyloid-positive group from the stable but not the progressive amyloid-negative group. On affective questionnaires, the stable amyloid-negative group reported significantly higher levels of depression than the amyloid-positive group. In our clinical cohort, visuospatial dysfunction and working memory impairment were better indicators of amyloid positivity than episodic memory dysfunction. These findings highlight the limited value of isolated cognitive scores in patients with atypical clinical presentation, comorbidities and/or early age of onset.
Keywords: Alzheimer’s disease; amyloid PET imaging; cognitive testing; dementia; neuropsychology.
© The Author(s) (2021). Published by Oxford University Press on behalf of the Guarantors of Brain.
Figures
References
-
- Kolanko MA, Malhotra PA.. Exploring Alzheimer’s disease subtypes at the prodromal stage. Brain. 2018;141(12):3285–3287. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources