

Feasibility study of hospital antimicrobial stewardship analytics using electronic health records
- PMID: 34223095
- PMCID: PMC8210026
- DOI: 10.1093/jacamr/dlab018
Feasibility study of hospital antimicrobial stewardship analytics using electronic health records
Abstract
Background: Hospital antimicrobial stewardship (AMS) programmes are multidisciplinary initiatives to optimize antimicrobial use. Most hospitals depend on time-consuming manual audits to monitor clinicians' prescribing. But much of the information needed could be sourced from electronic health records (EHRs).
Objectives: To develop an informatics methodology to analyse characteristics of hospital AMS practice using routine electronic prescribing and laboratory records.
Methods: Feasibility study using electronic prescribing, laboratory and clinical coding records from adult patients admitted to six specialities at Queen Elizabeth Hospital, Birmingham, UK (September 2017-August 2018). The study involved: (i) a review of AMS standards of care; (ii) their translation into concepts measurable from commonly available EHRs; and (iii) a pilot application in an EHR cohort study (n = 61679 admissions).
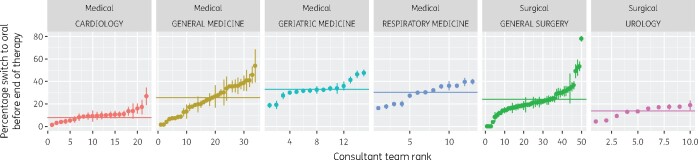
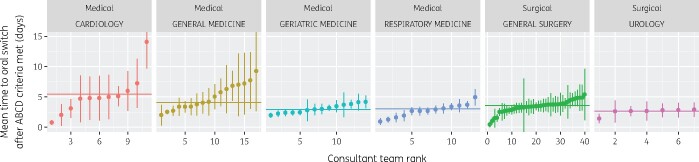
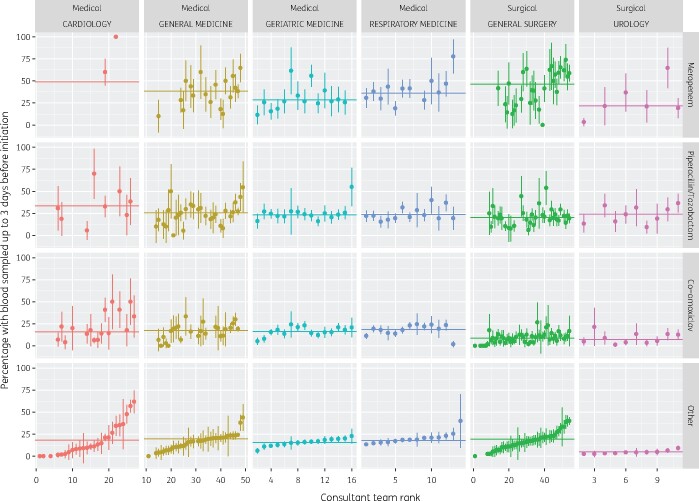
Results: We developed data modelling methods to characterize antimicrobial use (antimicrobial therapy episode linkage methods, therapy table, therapy changes). Prescriptions were linked into antimicrobial therapy episodes (mean 2.4 prescriptions/episode; mean length of therapy 5.8 days), enabling several actionable findings. For example, 22% of therapy episodes for low-severity community-acquired pneumonia were congruent with prescribing guidelines, with a tendency to use broader-spectrum antibiotics. Analysis of therapy changes revealed IV to oral therapy switching was delayed by an average 3.6 days (95% CI: 3.4-3.7). Microbial cultures were performed prior to treatment initiation in just 22% of antibacterial prescriptions. The proposed methods enabled fine-grained monitoring of AMS practice down to specialities, wards and individual clinical teams by case mix, enabling more meaningful peer comparison.
Conclusions: It is feasible to use hospital EHRs to construct rapid, meaningful measures of prescribing quality with potential to support quality improvement interventions (audit/feedback to prescribers), engagement with front-line clinicians on optimizing prescribing, and AMS impact evaluation studies.
© The Author(s) 2021. Published by Oxford University Press on behalf of the British Society for Antimicrobial Chemotherapy.
Figures

References
-
- Davey P, Sneddon J, Nathwani D.. Overview of strategies for overcoming the challenge of antimicrobial resistance. Expert Rev Clin Pharmacol 2010; 3: 667–86. - PubMed
-
- NICE. Antimicrobial Stewardship: Systems and Processes for Effective Antimicrobial Medicine Use. NICE guideline NG15. https://www.nice.org.uk/guidance/ng15. - PMC - PubMed
-
- SARI Hospital Antimicrobial Stewardship Working Group. Guidelines for Antimicrobial Stewardship in Hospitals in Ireland. https://www.hpsc.ie/a-z/microbiologyantimicrobialresistance/infectioncon....
-
- Haute Autorité de Santé. Antibiotic Therapy and Prevention of Bacterial Resistance in Healthcare Organisations. Clinical Practice Guideline 2008. https://www.has-sante.fr/jcms/c_665169/fr/strategie-d-antibiotherapie-et....
-
- Pulcini C, Binda F, Lamkang AS. et al. Developing core elements and checklist items for global hospital antimicrobial stewardship programmes: a consensus approach. Clin Microbiol Infect 2019; 25: 20–5. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources