

Closed-loop machine-controlled CPR system optimises haemodynamics during prolonged CPR
- PMID: 34223304
- PMCID: PMC8244522
- DOI: 10.1016/j.resplu.2020.100021
Closed-loop machine-controlled CPR system optimises haemodynamics during prolonged CPR
Abstract
Objectives: We evaluated the feasibility of optimising coronary perfusion pressure (CPP) during cardiopulmonary resuscitation (CPR) with a closed-loop, machine-controlled CPR system (MC-CPR) that sends real-time haemodynamic feedback to a set of machine learning and control algorithms which determine compression/decompression characteristics over time.
Background: American Heart Association CPR guidelines (AHA-CPR) and standard mechanical devices employ a "one-size-fits-all" approach to CPR that fails to adjust compressions over time or individualise therapy, thus leading to deterioration of CPR effectiveness as duration exceeds 15-20 min.
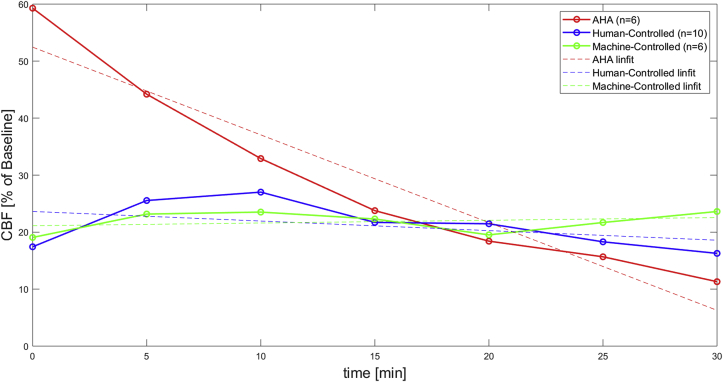
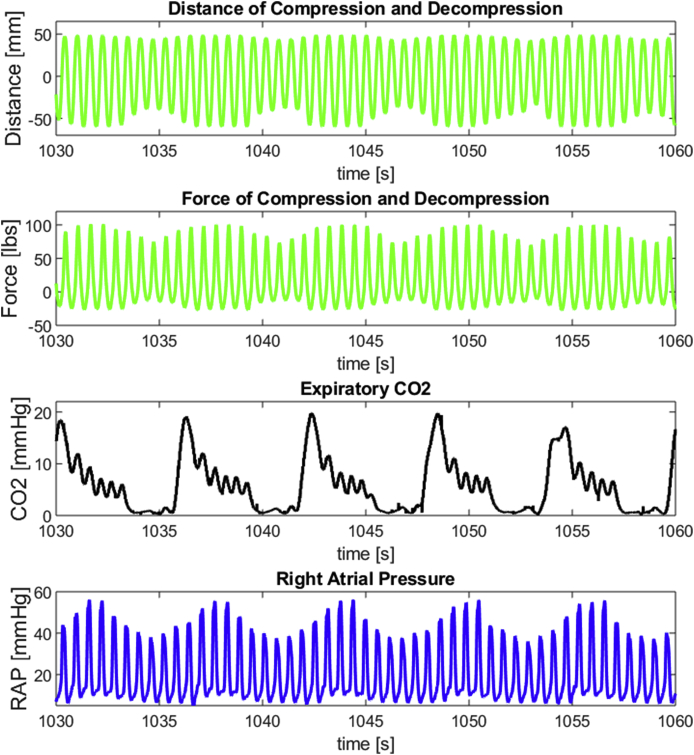
Methods: CPR was administered for 30 min in a validated porcine model of cardiac arrest. Intubated anaesthetised pigs were randomly assigned to receive MC-CPR (6), mechanical CPR conducted according to AHA-CPR (6), or human-controlled CPR (HC-CPR) (10). MC-CPR directly controlled the CPR piston's amplitude of compression and decompression to maximise CPP over time. In HC-CPR a physician controlled the piston amplitudes to maximise CPP without any algorithmic feedback, while AHA-CPR had one compression depth without adaptation.
Results: MC-CPR significantly improved CPP throughout the 30-min resuscitation period compared to both AHA-CPR and HC-CPR. CPP and carotid blood flow (CBF) remained stable or improved with MC-CPR but deteriorated with AHA-CPR. HC-CPR showed initial but transient improvement that dissipated over time.
Conclusion: Machine learning implemented in a closed-loop system successfully controlled CPR for 30 min in our preclinical model. MC-CPR significantly improved CPP and CBF compared to AHA-CPR and ameliorated the temporal haemodynamic deterioration that occurs with standard approaches.
Keywords: CPR; Cardiopulmonary resuscitation; Haemodynamics; Machine learning; Mechanical CPR; OHCA; Personalized medicine; Porcine; Refractory VF.
© 2020 The Authors.
Conflict of interest statement
None of the authors had any conflicts of interest or financial disclosures to declare.
Figures



References
-
- Virani S.S., Alonso A., Benjamin E.J. Heart disease and stroke statistics update: a report from the American Heart Association. Circulation. 2020;141:e139–e596. - PubMed
-
- Zive D.M., Schmicker R., Daya M. Survival and variability over time from out of hospital cardiac arrest across large geographically diverse communities participating in the Resuscitation Outcomes Consortium. Resuscitation. 2018;131:74–82. - PubMed
-
- Grunau B., Puyat J., Wong H. Gains of continuing resuscitation in refractory out-of-hospital cardiac arrest: a model-based analysis to identify deaths due to intra-arrest prognostication. Prehosp Emerg Care. 2018;22:198–207. - PubMed
-
- Nagao K., Nonogi H., Yonemoto N. Duration of prehospital resuscitation efforts after out-of-hospital cardiac arrest. Circulation. 2016;133:1386–1396. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
