

The physiologic response to rescue therapy with vasopressin versus epinephrine during experimental pediatric cardiac arrest
- PMID: 34223324
- PMCID: PMC8244440
- DOI: 10.1016/j.resplu.2020.100050
The physiologic response to rescue therapy with vasopressin versus epinephrine during experimental pediatric cardiac arrest
Abstract
Aim: Compare vasopressin to a second dose of epinephrine as rescue therapy after ineffective initial doses of epinephrine in diverse models of pediatric in-hospital cardiac arrest.
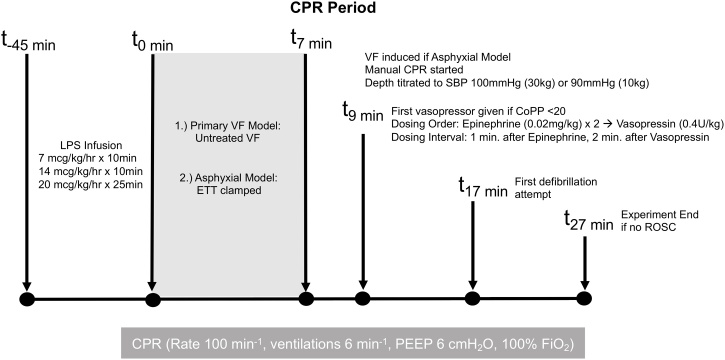
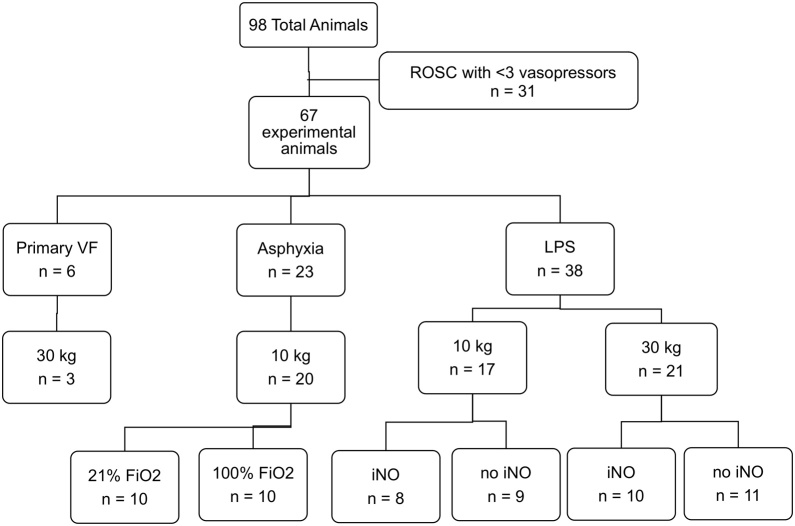
Methods: 67 one- to three-month old female swine (10-30 kg) in six experimental cohorts from one laboratory received hemodynamic-directed CPR, a resuscitation method where high quality chest compressions are provided and vasopressor administration is titrated to coronary perfusion pressure (CoPP) ≥20 mmHg. Vasopressors are given when CoPP is <20 mmHg, in sequences of two doses of 0.02 mg/kg epinephrine separated by minimum one-minute, then a rescue dose of 0.4 U/kg vasopressin followed by minimum two-minutes. Invasive measurements were used to evaluate and compare the hemodynamic and neurologic effects of each vasopressor dose.
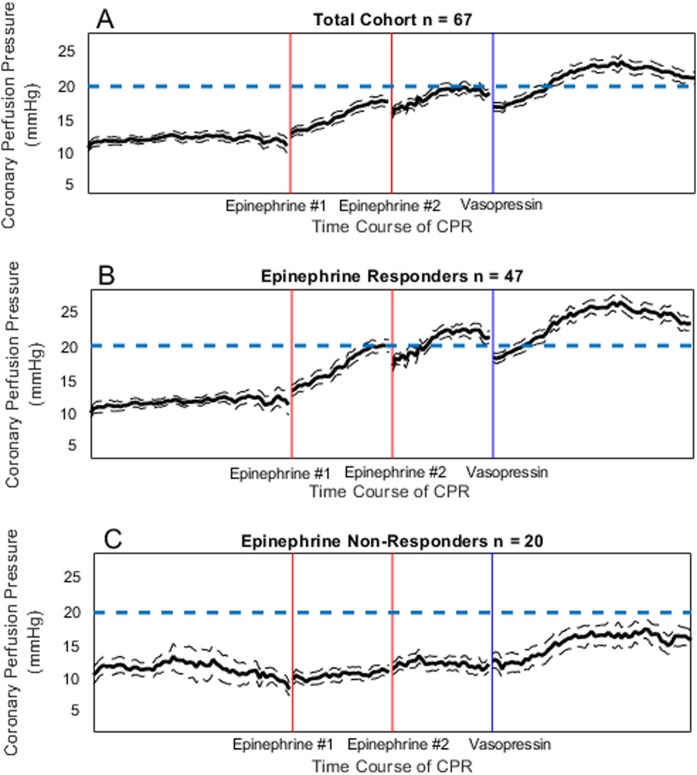
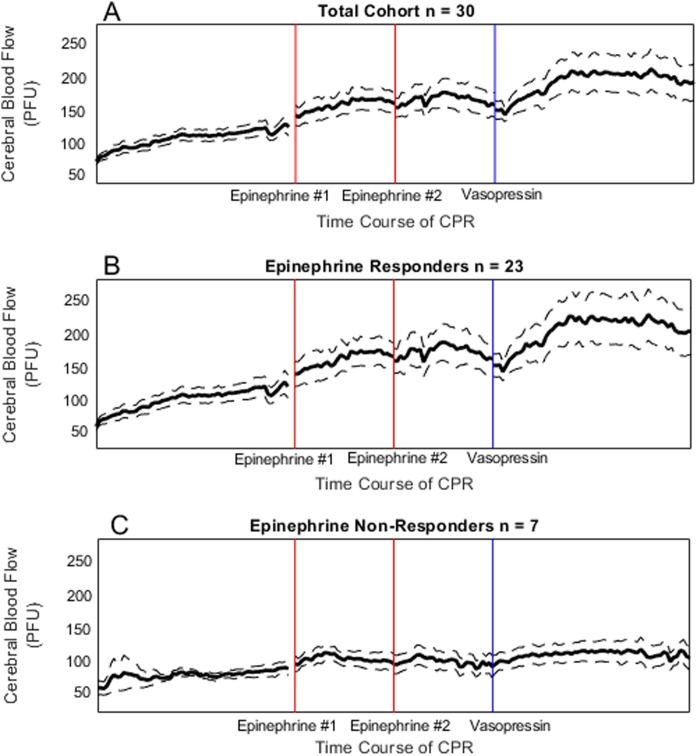
Results: Increases in CoPP and cerebral blood flow (CBF) were greater with vasopressin rescue than epinephrine rescue (CoPP: +8.16 [4.35, 12.06] mmHg vs. + 5.43 [1.56, 9.82] mmHg, p = 0.02; CBF: +14.58 [-0.05, 38.12] vs. + 0.00 [-0.77, 18.24] perfusion units (PFU), p = 0.005). Twenty animals (30%) failed to achieve CoPP ≥20 mmHg after two doses of epinephrine; 9/20 (45%) non-responders achieved CoPP ≥20 mmHg after vasopressin. Among all animals, the increase in CBF was greater with vasopressin (+14.58 [-0.58, 38.12] vs. 0.00 [-0.77, 18.24] PFU, p = 0.005).
Conclusions: CoPP and CBF rose significantly more after rescue vasopressin than after rescue epinephrine. Importantly, CBF increased after vasopressin rescue, but not after epinephrine rescue. In the 30% that failed to meet CoPP of 20 mmHg after two doses of epinephrine, 45% achieved target CoPP with a single rescue vasopressin dose.
Keywords: Cardiac arrest; Cardiopulmonary resuscitation; Cerebral blood flow; Coronary perfusion pressure; Epinephrine; Pediatrics; Vasopressin.
© 2020 The Authors.
Figures
References
-
- Paradis N.A., Martin G.B. Coronary perfusion pressure and the return of spontaneous circulation in human cardiopulmonary resuscitation. JAMA. 1990;263:1106–1113. - PubMed
-
- Berg R.A., Sanders A.B., Kern K.B. Adverse hemodynamic effects of interrupting chest compressions for rescue breathing during cardiopulmonary resuscitation for ventricular fibrillation cardiac arrest. Circulation. 2001;104:2465–2470. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
