

Every one-minute delay in EMS on-scene resuscitation after out-of-hospital pediatric cardiac arrest lowers ROSC by 5
- PMID: 34223334
- PMCID: PMC8244411
- DOI: 10.1016/j.resplu.2020.100062
Every one-minute delay in EMS on-scene resuscitation after out-of-hospital pediatric cardiac arrest lowers ROSC by 5
Abstract
Objective: To determine which aspects of prehospital care impact outcomes after pediatric cardiac arrest.
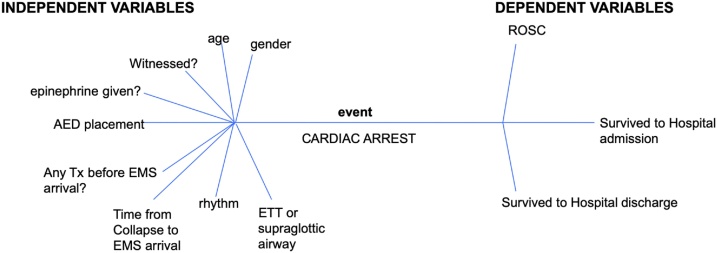
Methods: In this study, the authors examine 5 years of consecutive data from their county emergency medical system (EMS), to identify predictors of good outcome after pediatric cardiac arrest, including return of spontaneous circulation (ROSC), survival to hospital admission (HA) and survival to hospital discharge (HD). Three logistic regression models were performed using JMP 14.1 Pro for Windows, each with the following nine predictors: age, sex, ventilation method (endotracheal intubation vs. supraglottic airway), initial rhythm (pulseless electrical activity vs. asystole), epinephrine administration, bystander treatment prior to EMS arrival, time from collapse to EMS arrival, automatic external defibrillator (AED) placement, and whether the arrest was witnessed. Odds ratio confidence intervals were calculated using the Wald method, and corresponding p-values were obtained with the likelihood ratio χ2 test.
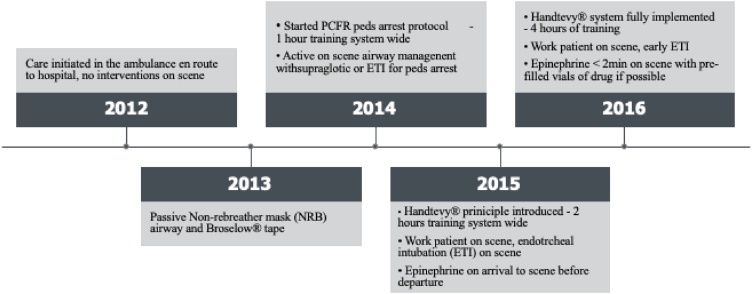
Results: From January 1, 2012 to December 31, 2016, there were 133 pediatric cardiac arrests, of which we had complete data on 109 patients for pediatric cardiac arrest. The median age was 8 months, with an IQR of 2.25-24 months, and a range of 0-108 months (0-9 years). There was return of spontaneous circulation (ROSC) in 20% of cases overall, with 16% making it to hospital admission, and 9% making it alive out of the hospital.The median time to EMS arrival for witnessed events was 10 min, with an interquartile range (IQR) of 6.5-16 min, and a range of 0-25 min. The median time to EMS arrival for unwitnessed events was 30 min, with an IQR of 19-62.5 min, and a range of 9-490 min.Predictors of ROSC included epinephrine administration (p = .00007), bystander treatment before EMS arrival (p = .0018), older age (p = .0025), shorter time to EMS arrival (p = .0048), and AED placement. Predictors of hospital admission included epinephrine NOT being administered (p = .0004), bystander treatment before EMS arrival (p = .0088), shorter time to EMS arrival (p = .0141), and AED placement (p = .0062). The only significant predictor of survival to hospital discharge alive that was identified was shorter time to EMS arrival (p = .0014), as there was insufficient data for many of the predictor variables in this analysis.
Conclusion: Shorter time to EMS arrival from time of arrest, any bystander treatment prior to EMS arrival, and AED placement resulted in significantly higher rates of return of spontaneous circulation. Epinephrine administration significantly improved ROSC, but had the opposite effect on HA. Only shorter time to EMS arrival from time of arrest was significantly associated with survival to hospital discharge. Each additional minute for the EMS to arrive resulted in 5% decreased odds of ROSC and hospital admission, and 12% decreased odds of surviving to hospital discharge.
Keywords: AED, automated external defibrillator; AHA, American Heart Association; BVM, bag-valve mask; CPR; CPR, cardiopulmonary resuscitation; EMS, emergency medical services; ETT, endotracheal intubation; HA, hospital admission; HD, discharged alive from the hospital; IHCA, in hospital cardiac arrest; NRM, non-rebreather mask; OHCA, out of hospital cardiac arrest; PEA, pulseless electrical activity; Pediatric cardiac arrest; ROSC, return of spontaneous circulation; Resuscitation.
© 2020 The Authors.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- Nadkarni V.M., Larkin G.L., Peberdy M.A. National Registry of Cardiopulmonary Resuscitation Investigators. First documented rhythm and clinical outcome from in-hospital cardiac arrest among children and adults. JAMA. 2006;295(January (1)):50–57. doi: 10.1001/jama.295.1.50. PMID: 16391216. - DOI - PubMed
-
- Harris M., Patterson J., Morse J. Doctors, nurses, and parents are equally poor at estimating pediatric weights. Pediatric Emergency Care. 1999;15(1):17–18. - PubMed
-
- Kleinman Monica E., Chameides Leon, Schexnayder Stephen M. 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2010;122:S876–S908. - PubMed
-
- Young K.D., Seidel J.S. Pediatric cardiopulmonary resuscitation: a collective review. Ann Emerg Med. 1999;33:195–205. - PubMed
LinkOut - more resources
Full Text Sources
