

FDA-authorized mRNA COVID-19 vaccines are effective per real-world evidence synthesized across a multi-state health system
- PMID: 34223401
- PMCID: PMC8238652
- DOI: 10.1016/j.medj.2021.06.007
FDA-authorized mRNA COVID-19 vaccines are effective per real-world evidence synthesized across a multi-state health system
Abstract
Background: Two US Food and Drug Administration (FDA)-authorized coronavirus disease 2019 (COVID-19) mRNA vaccines, BNT162b2 (Pfizer/BioNTech) and mRNA-1273 (Moderna), have demonstrated high efficacy in large phase 3 randomized clinical trials. It is important to assess their effectiveness in a real-world setting.
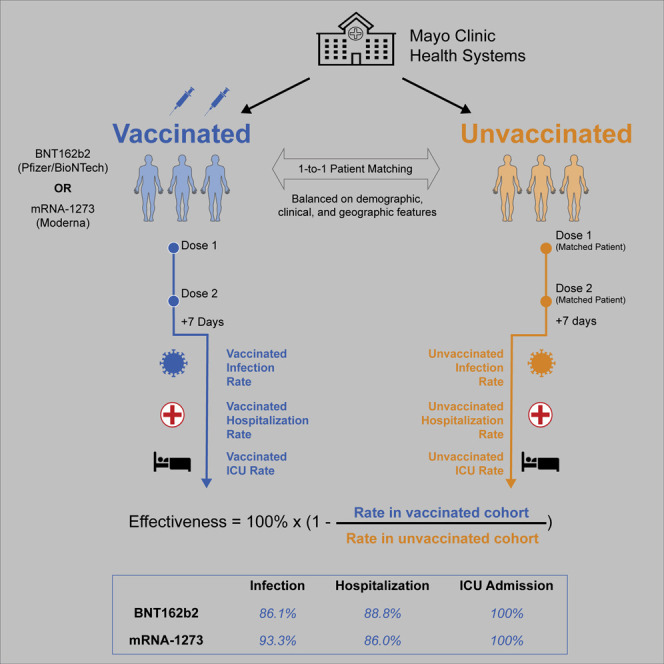
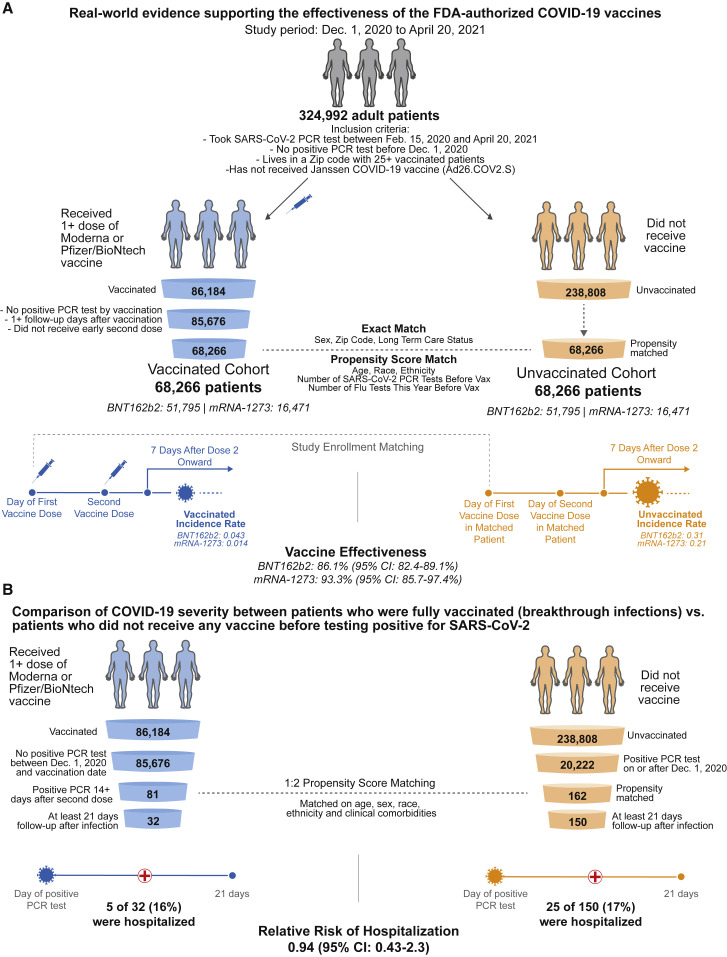
Methods: This is a retrospective analysis of 136,532 individuals in the Mayo Clinic health system (Arizona, Florida, Iowa, Minnesota, and Wisconsin) with PCR testing data between December 1, 2020 and April 20, 2021. We compared clinical outcomes for a vaccinated cohort of 68,266 individuals who received at least one dose of either vaccine (nBNT162b2 = 51,795; nmRNA-1273 = 16,471) and an unvaccinated control cohort of 68,266 individuals propensity matched based on relevant demographic, clinical, and geographic features. We estimated real-world vaccine effectiveness by comparing incidence rates of positive severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) PCR testing and COVID-19-associated hospitalization and intensive care unit (ICU) admission starting 7 days after the second vaccine dose.
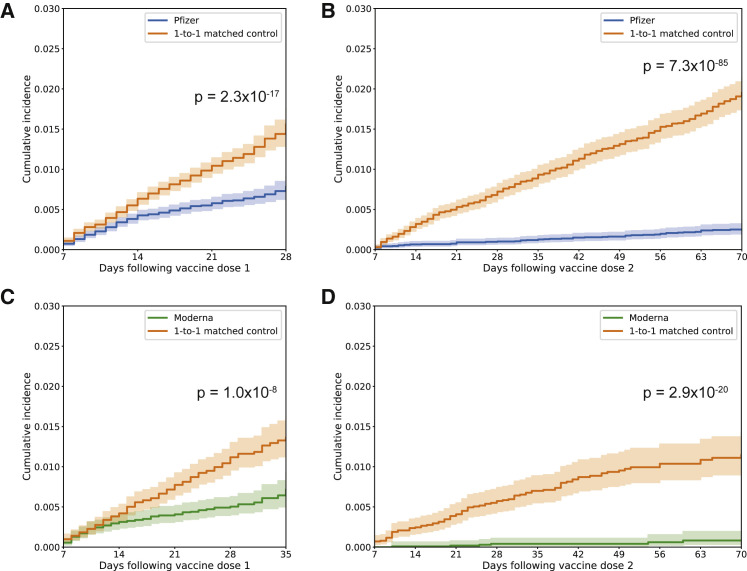
Findings: The real-world vaccine effectiveness of preventing SARS-CoV-2 infection was 86.1% (95% confidence interval [CI]: 82.4%-89.1%) for BNT162b2 and 93.3% (95% CI: 85.7%-97.4%) for mRNA-1273. BNT162b2 and mRNA-1273 were 88.8% (95% CI: 75.5%-95.7%) and 86.0% (95% CI: 71.6%-93.9%) effective in preventing COVID-19-associated hospitalization. Both vaccines were 100% effective (95% CIBNT162b2: 51.4%-100%; 95% CImRNA-1273: 43.3%-100%) in preventing COVID-19-associated ICU admission.
Conclusions: BNT162b2 and mRNA-1273 are effective in a real-world setting and are associated with reduced rates of SARS-CoV-2 infection and decreased burden of COVID-19 on the healthcare system.
Funding: This study was funded by nference.
Keywords: COVID-19; COVID-19 vaccines; propensity score matching; real world evidence.
© 2021 Elsevier Inc.
Conflict of interest statement
C.P., P.L., A.P., V.A., A.V., M.J.M.N., and V.S. are employees of nference and have financial interests in the company and in the successful application of this research. J.C.O. receives personal fees from Elsevier and Bates College and small grants from nference, Inc., outside of the submitted work. A.D.B. is a consultant for Abbvie, is on scientific advisory boards for nference and Zentalis, and is founder and President of Splissen Therapeutics. J.H., J.C.O., M.D.S., A.V., and A.D.B. are employees of the Mayo Clinic. The Mayo Clinic may stand to gain financially from the successful outcome of the research. nference collaborates with Janssen and other bio-pharmaceutical companies on data science initiatives unrelated to this study. These collaborations had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. This research has been reviewed by the Mayo Clinic Conflict of Interest Review Board and is being conducted in compliance with Mayo Clinic Conflict of Interest policies.
Figures
References
-
- Johns Hopkins Coronavirus Resource Center . 2021. COVID-19 Dashboard.https://coronavirus.jhu.edu/map.html
-
- Lan J., Ge J., Yu J., Shan S., Zhou H., Fan S., Zhang Q., Shi X., Wang Q., Zhang L., Wang X. Structure of the SARS-CoV-2 spike receptor-binding domain bound to the ACE2 receptor. Nature. 2020;581:215–220. - PubMed
-
- Venkatakrishnan A.J., Puranik A., Anand A., Zemmour D., Yao X., Wu X., Chilaka R., Murakowski D.K., Standish K., Raghunathan B., et al. Knowledge synthesis of 100 million biomedical documents augments the deep expression profiling of coronavirus receptors. (2020. eLife. 2020;9:e58040. - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
