

Polytrauma Is Associated with Increased Three- and Six-Month Disability after Traumatic Brain Injury: A TRACK-TBI Pilot Study
- PMID: 34223528
- PMCID: PMC8240880
- DOI: 10.1089/neur.2020.0004
Polytrauma Is Associated with Increased Three- and Six-Month Disability after Traumatic Brain Injury: A TRACK-TBI Pilot Study
Abstract
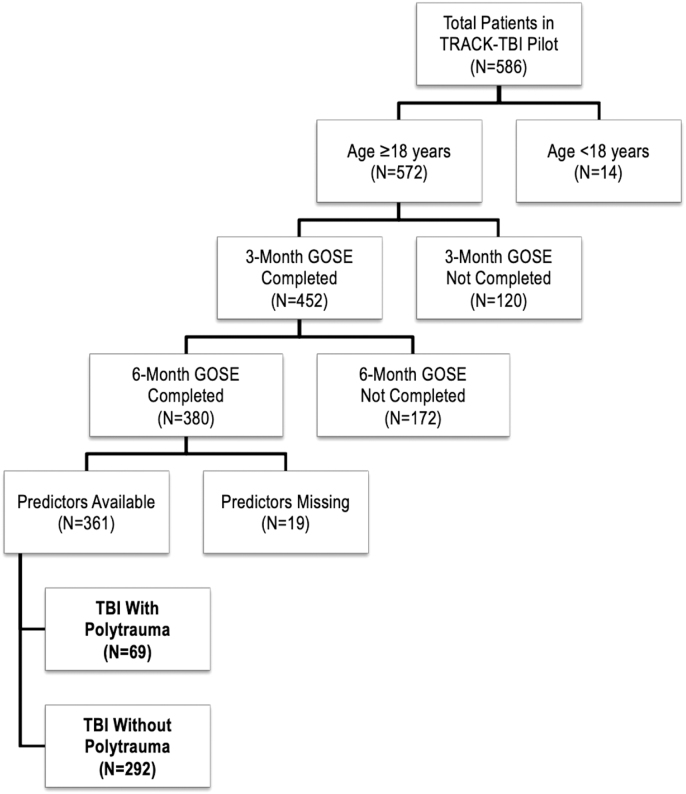
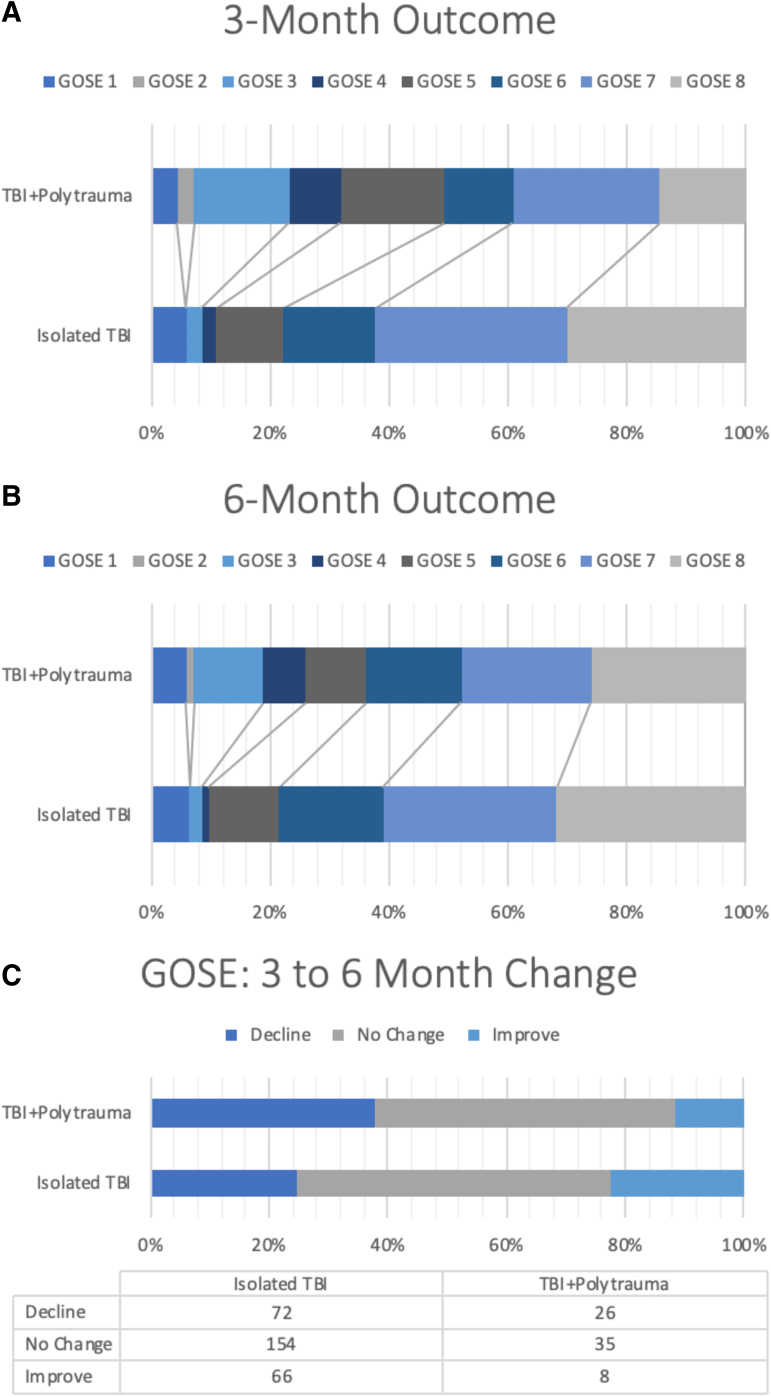
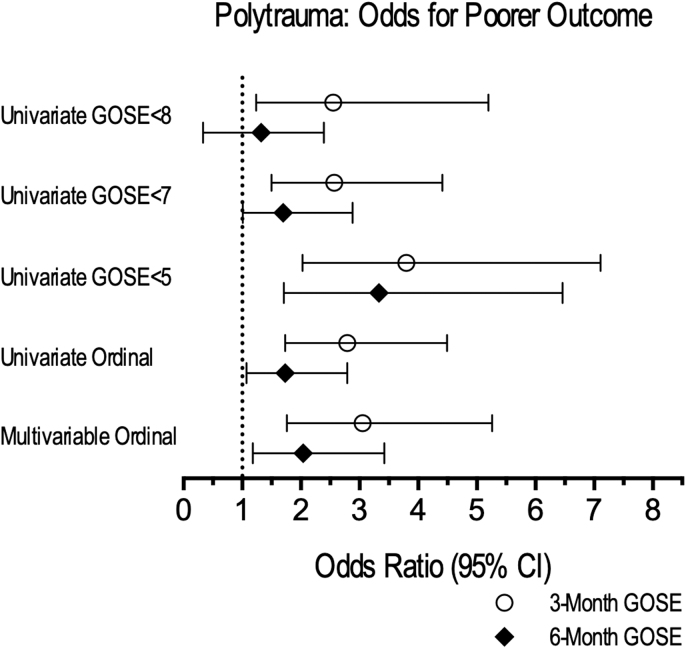
Polytrauma and traumatic brain injury (TBI) frequently co-occur and outcomes are routinely measured by the Glasgow Outcome Scale-Extended (GOSE). Polytrauma may confound GOSE measurement of TBI-specific outcomes. Adult patients with TBI from the prospective Transforming Research and Clinical Knowledge in Traumatic Brain Injury Pilot (TRACK-TBI Pilot) study had presented to a Level 1 trauma center after injury, received head computed tomography (CT) within 24 h, and completed the GOSE at 3 months and 6 months post-injury. Polytrauma was defined as an Abbreviated Injury Score (AIS) ≥3 in any extracranial region. Univariate regressions were performed using known GOSE clinical cutoffs. Multi-variable regressions were performed for the 3- and 6-month GOSE, controlling for known demographic and injury predictors. Of 361 subjects (age 44.9 ± 18.9 years, 69.8% male), 69 (19.1%) suffered polytrauma. By Glasgow Coma Scale (GCS) assessment, 80.1% had mild, 5.8% moderate, and 14.1% severe TBI. On univariate logistic regression, polytrauma was associated with increased odds of moderate disability or worse (GOSE ≤6; 3 month odds ratio [OR] = 2.57 [95% confidence interval (CI): 1.50-4.41; 6 month OR = 1.70 [95% CI: 1.01-2.88]) and death/severe disability (GOSE ≤4; 3 month OR = 3.80 [95% CI: 2.03-7.11]; 6 month OR = 3.33 [95% CI: 1.71-6.46]). Compared with patients with isolated TBI, more polytrauma patients experienced a decline in GOSE from 3 to 6 months (37.7 vs. 24.7%), and fewer improved (11.6 vs. 22.6%). Polytrauma was associated with greater univariate ordinal odds for poorer GOSE (3 month OR = 2.79 [95% CI: 1.73-4.49]; 6 month OR = 1.73 [95% CI: 1.07-2.79]), which was conserved on multi-variable ordinal regression (3 month OR = 3.05 [95% CI: 1.76-5.26]; 6 month OR = 2.04 [95% CI: 1.18-3.42]). Patients with TBI with polytrauma are at greater risk for 3- and 6-month disability compared with those with isolated TBI. Methodological improvements in assessing TBI-specific disability, versus disability attributable to all systemic injuries, will generate better TBI outcomes assessment tools.
Keywords: disability; functional outcome; outcome measure; polytrauma; traumatic brain injury.
© John K. Yue et al., 2020; Published by Mary Ann Liebert, Inc.
Conflict of interest statement
No competing financial interests exist.
Figures
References
-
- Maas, A.I.R., Menon, D.K., Adelson, P.D., Andelic, N., Bell, M.J., Belli, A., Bragge, P., Brazinova, A., Büki, A., Chesnut, R.M., Citerio, G., Coburn, M., Cooper, D.J., Crowder, A.T., Czeiter, E., Czosnyka, M., Diaz-Arrastia, R., Dreier, J.P., Duhaime, A.-C., Ercole, A., van Essen, T.A., Feigin, V.L., Gao, G., Giacino, J., Gonzalez-Lara, L.E., Gruen, R.L., Gupta, D., Hartings, J.A., Hill, S., Jiang, J.-Y., Ketharanathan, N., Kompanje, E.J.O., Lanyon, L., Laureys, S., Lecky, F., Levin, H., Lingsma, H.F., Maegele, M., Majdan, M., Manley, G., Marsteller, J., Mascia, L., McFadyen, C., Mondello, S., Newcombe, V., Palotie, A., Parizel, P.M., Peul, W., Piercy, J., Polinder, S., Puybasset, L., Rasmussen, T.E., Rossaint, R., Smielewski, P., Söderberg, J., Stanworth, S.J., Stein, M.B., von Steinbüchel, N., Stewart, W., Steyerberg, E.W., Stocchetti, N., Synnot, A., TeAo, B., Tenovuo, O., Theadom, A., Tibboel, D., Videtta, W., Wang, K.K.W., Williams, W.H., Wilson, L., Yaffe, K., and InTBIR Participants and Investigators. (2017). Traumatic brain injury: integrated approaches to improve prevention, clinical care, and research. Lancet Neurol. 16, 987–1048 - PubMed
-
- Xydakis, M.S., Ling, G.S.F., Mulligan, L.P., Olsen, C.H., and Dorlac, W.C. (2012). Epidemiologic aspects of traumatic brain injury in acute combat casualties at a major military medical center: a cohort study. Ann. Neurol. 72, 673–681 - PubMed
-
- Yuan, Q., Liu, H., Wu, X., Sun, Y., Yao, H., Zhou, L., and Hu, J. (2012). Characteristics of acute treatment costs of traumatic brain injury in Eastern China–a multi-centre prospective observational study. Injury 43, 2094–2099 - PubMed