

Reactivation of Vogt-Koyanagi-Harada disease under control for more than 6 years, following anti-SARS-CoV-2 vaccination
- PMID: 34224024
- PMCID: PMC8256412
- DOI: 10.1186/s12348-021-00251-5
Reactivation of Vogt-Koyanagi-Harada disease under control for more than 6 years, following anti-SARS-CoV-2 vaccination
Abstract
Background/purpose: Vogt-Koyanagi-Harada (VKH) disease is a primary stromal choroiditis with bilateral granulomatous panuveitis. If initial-onset VKH is treated early and relentlessly the disease can be controlled and even "cured" in a substantial number of cases. We are reporting on a patient treated early and in a sustained fashion who was inflammation free for seven years but who presented a reactivation 6 weeks after the second dose of anti-SARS-CoV-2 vaccination.
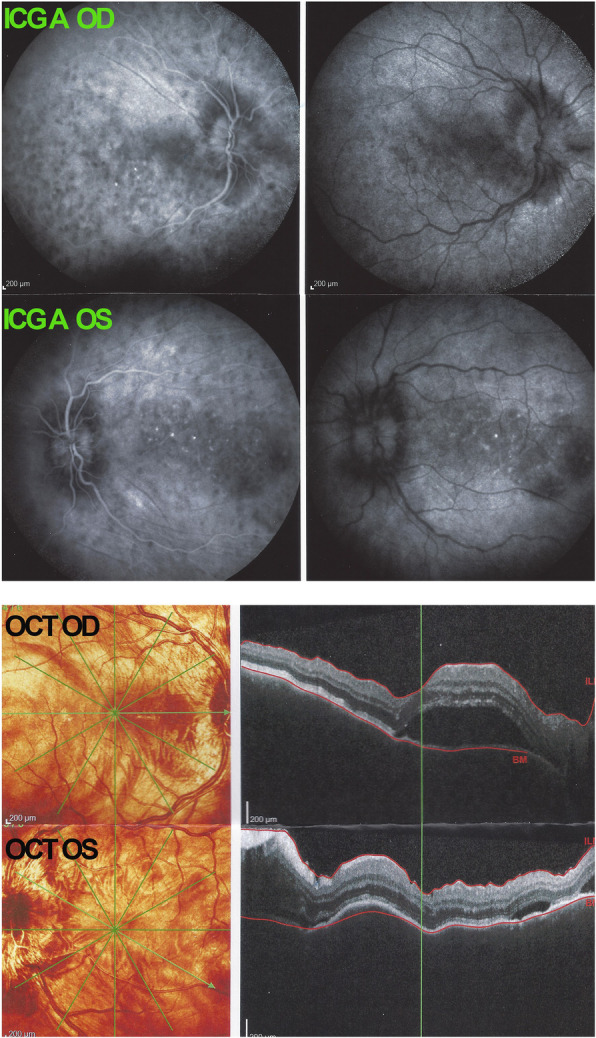
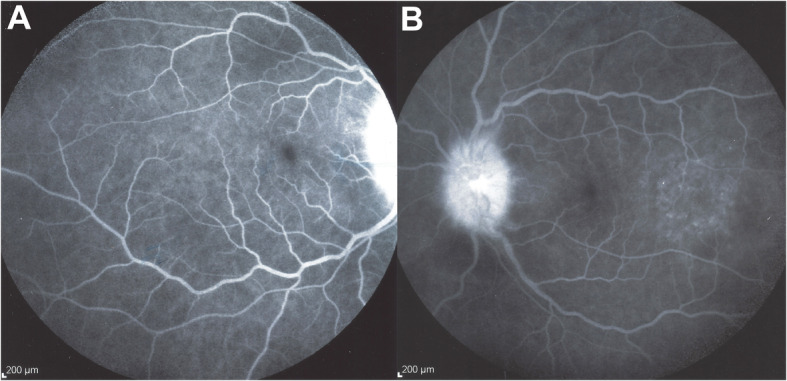
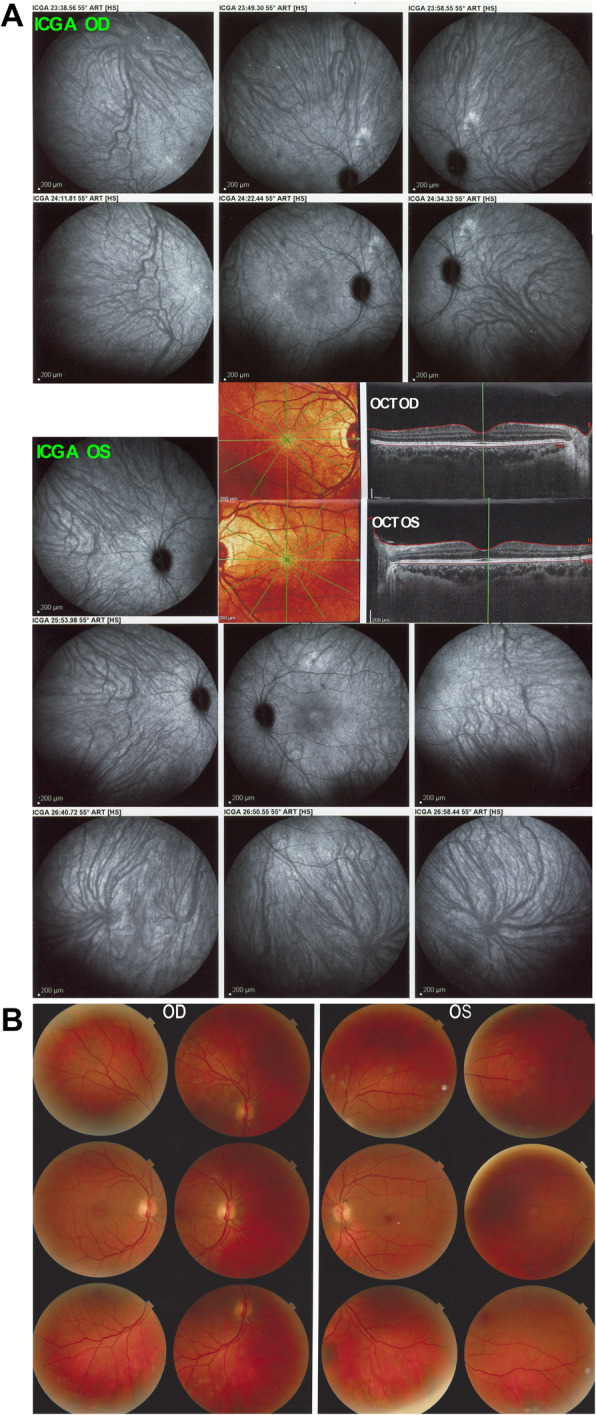
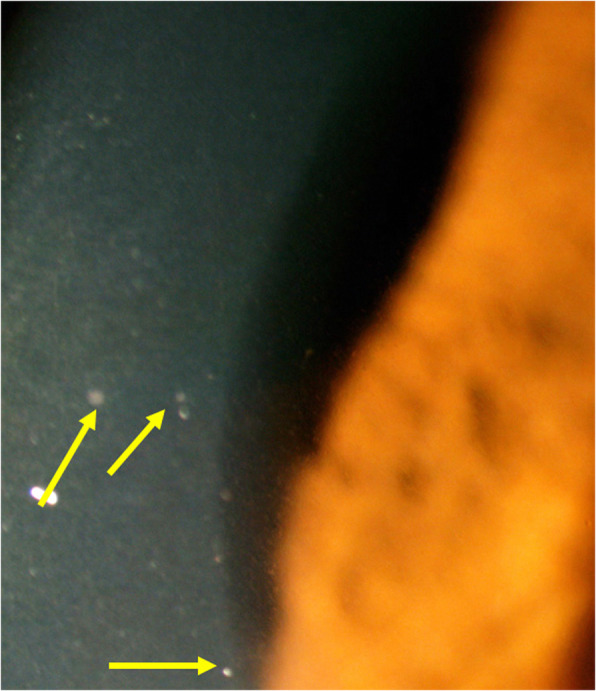
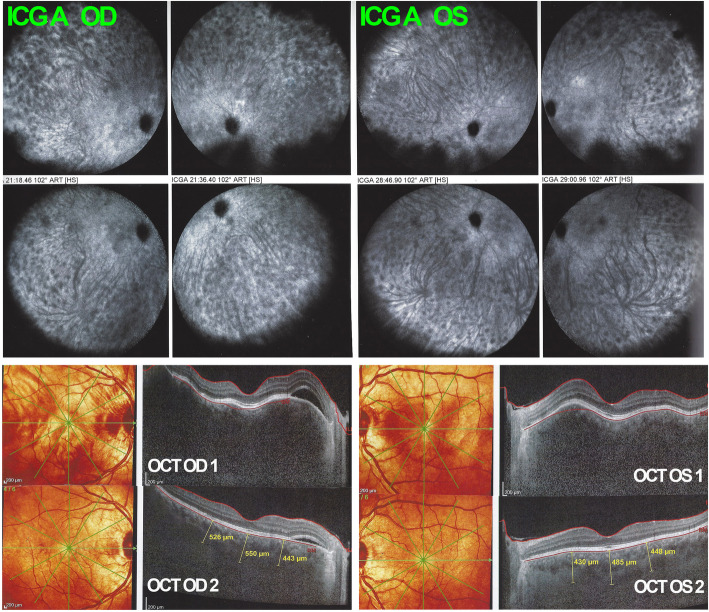
Case report: A 43-year-old woman presented with severe initial-onset VKH disease which was brought under control using steroidal and non-steroidal Immunosuppression (mycophenolic acid and cyclosporine) with additional infliximab infusions because of the persistence of subclinical choroiditis identified on ICGA. Under infliximab alone disease had been inflammation free with no subclinical disease and absence of sunset glow fundus for 6 years. However, following anti-SARS-CoV-2 vaccination, severe resurgence of the disease occurred with exudative retinal detachments. Disease was rapidly brought again under control with oral prednisone (1 mg/kg) therapy and a new loading scheme of infliximab therapy.
Conclusion: VKH disease results from an autoimmune process directed against melanocyte associated antigens which can be controlled when early and sustained immunosuppressive treatment is introduced. It seems that anti-SARS-CoV-2 vaccination can be at the origin of reactivation of long-time controlled disease.
Keywords: Anti-SARS-CoV-2 vaccination; Autoimmune stromal choroiditis; Vogt-Koyanagi-Harada disease: Indocyanine green angiography.
Conflict of interest statement
No conflict of interest.
Figures

References
-
- Bouchenaki N, Herbort CP. Stromal choroiditis. In: Pleyer U, Mondino B, editors. Essentials in Ophthalmology: Uveitis and Immunological Disorders. Berlin, Heidelberg, New York: Springer; 2004. pp. 234–253.
-
- Gocho K, Kondo I, Yamaki K. Identification of autoreactive T cells in Vogt-Koyanagi-Harada disease. Invest Ophthalmol Vis Sci. 2001;42(9):2004–2009. - PubMed
-
- Attia S, Khochtali S, Kahloum R, Zouali S, Khairallah M. Vogt-Koyanagi-Harada disease. Expert Rev Ophthalmol. 2012;7(6):565–585. doi: 10.1586/eop.12.63. - DOI
LinkOut - more resources
Full Text Sources
Miscellaneous
