

Definition and Prediction of Early Recurrence and Mortality Following Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy for Colorectal Peritoneal Metastases: Towards Predicting Oncologic Futility Preoperatively
- PMID: 34224045
- PMCID: PMC8666126
- DOI: 10.1245/s10434-021-10289-3
Definition and Prediction of Early Recurrence and Mortality Following Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy for Colorectal Peritoneal Metastases: Towards Predicting Oncologic Futility Preoperatively
Abstract
Introduction: Early recurrence (ER) is a significant challenge for patients with colorectal peritoneal metastases (CRPM) following cytoreductive surgery with hyperthermic intraperitoneal chemotherapy (CRS HIPEC). Preoperative risk stratification for ER would improve preoperative decision making.
Methods: We conducted a retrospective study examining patients who underwent CRS HIPEC for CRPM from 2000 to 2018. Optimal definition of ER was determined via minimum p-value approach based on differentiation of post-recurrence survival. Risk factors for ER were assessed in a derivation cohort by uni- and multivariate logistic regression. A predictive score for ER was generated using preoperative variables and validated in an independent cohort.
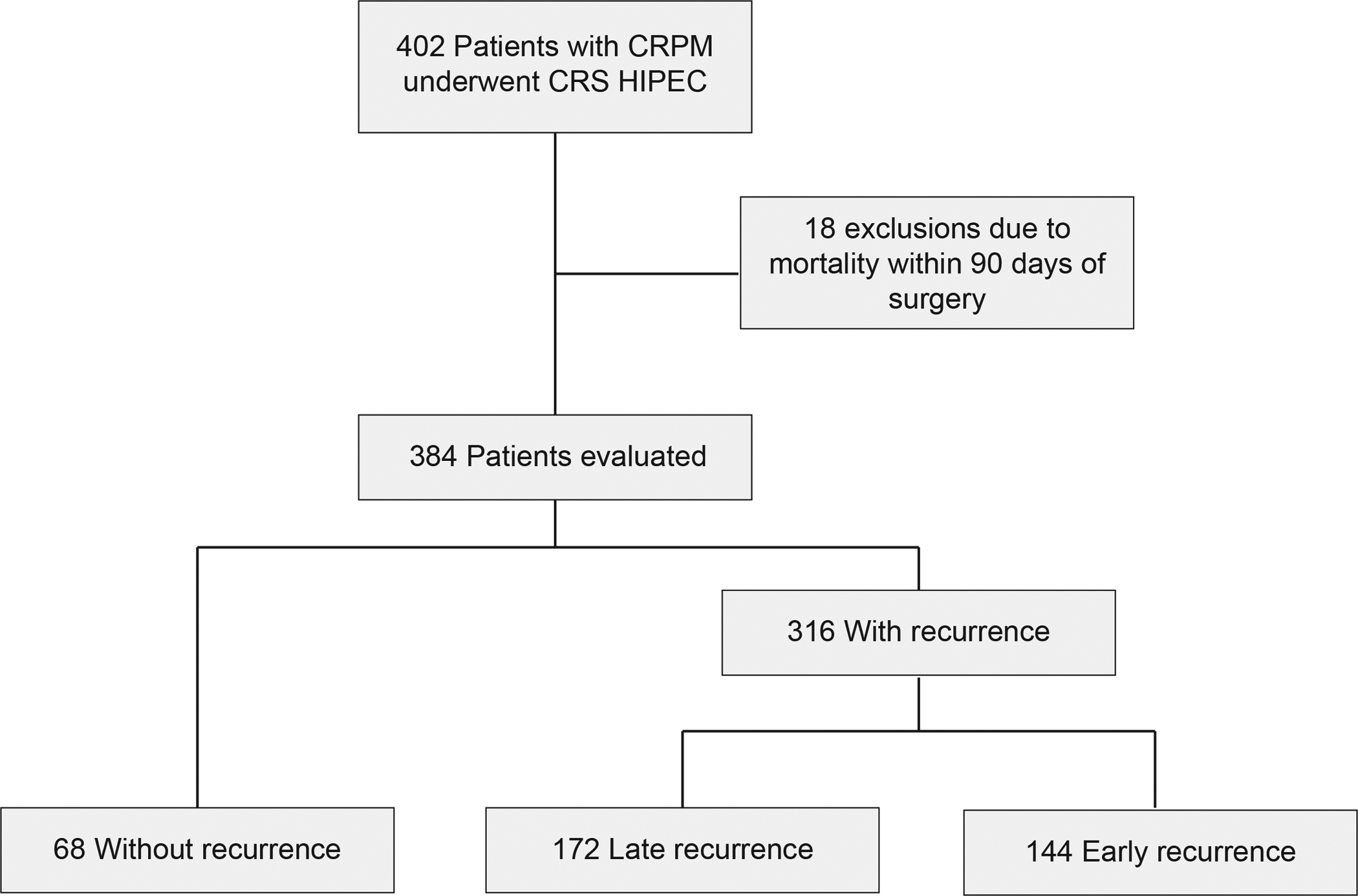
Results: 384 patients were analyzed, 316 (82%) had documented recurrence. Optimal length of post-operative RFS to distinguish ER (n = 144, 46%) vs. late recurrence (LR) (n = 172, 63%) was 8 mos (p<0.01). ER patients had shorter median OS post-CRS-HIPEC (13.6 vs. 39.4 mos, p<0.01). Preoperative BMI (OR 1.88), liver lesions (OR 1.89), progression on chemotherapy (OR 2.14), positive lymph nodes (OR 2.47) and PCI score (16-20: OR 1.7; >20: OR 4.37) were significant predictors of ER (all p<0.05). Using this model, patients were assigned risk scores from 0 to 9. Intermediate (scores 4-6) and high-risk patients (score 7-9) had observed rates of ER of 56% and 79% and overall 2-year survival rates of 27% and 0% respectively. The model showed fair discrimination (AUC 0.72) and good calibration (Hosmer-Lemeshow GOF p = 0.68).
Conclusions: ER predicts markedly worse OS following surgery. Preoperative factors can accurately stratify risk for ER and identify patients in whom CRS-HIPEC for CPRM is futile.
© 2021. Society of Surgical Oncology.
Figures

References
-
- Rahib L, Smith BD, Aizenberg R, Rosenzweig AB, Fleshman JM, Matrisian LM. Projecting cancer incidence and deaths to 2030: the unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer research. June 1 2014;74(11):2913–21. doi: 10.1158/0008-5472.Can-14-0155 - DOI - PubMed
-
- Franko J, Shi Q, Meyers JP, et al. Prognosis of patients with peritoneal metastatic colorectal cancer given systemic therapy: an analysis of individual patient data from prospective randomised trials from the Analysis and Research in Cancers of the Digestive System (ARCAD) database. The Lancet Oncology. December 2016;17(12):1709–1719. doi: 10.1016/s1470-2045(16)30500-9 - DOI - PubMed
-
- Quénet F, Elias D, Roca L, et al. Cytoreductive surgery plus hyperthermic intraperitoneal chemotherapy versus cytoreductive surgery alone for colorectal peritoneal metastases (PRODIGE 7): a multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. February 2021;22(2):256–266. doi: 10.1016/s1470-2045(20)30599-4 - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
