

Risk of Infection with Immune Checkpoint Inhibitors: A Systematic Review and Meta-analysis
- PMID: 34224061
- PMCID: PMC8256230
- DOI: 10.1007/s11523-021-00824-3
Risk of Infection with Immune Checkpoint Inhibitors: A Systematic Review and Meta-analysis
Abstract
Background: The relative risk (RR) of infection for patients treated with immune checkpoint inhibitors (ICIs) is unknown.
Objectives: This study evaluated the risk of infection for patients with solid tumors undergoing ICI therapy based on a systematic review and meta-analysis.
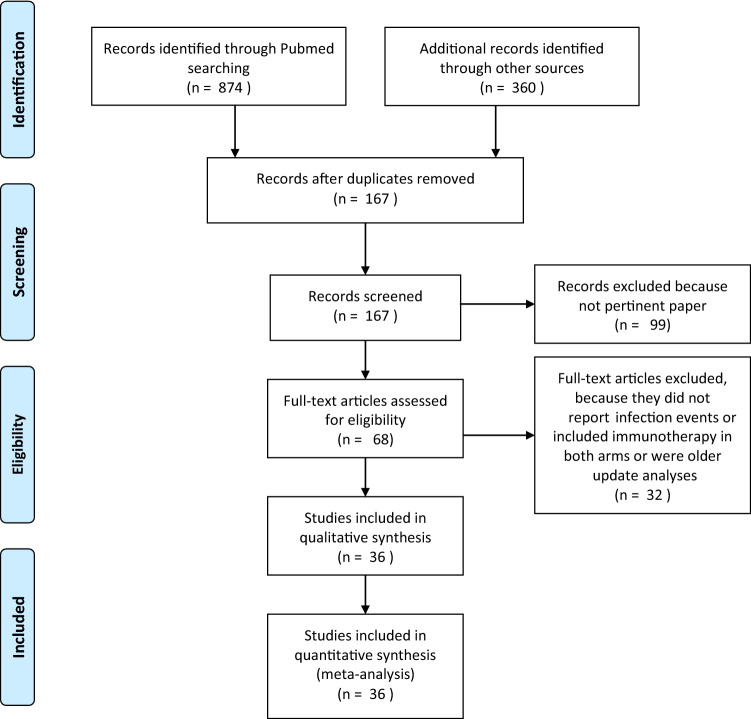
Patients and methods: The Cochrane Library, EMBASE, and Pubmed databases were searched up to 1 December 2020. Randomized trials comparing any ICI alone, with chemotherapy (CT), or with other agents versus placebo, CT, or other agents were included. Three independent reviewers extracted the data. The primary outcome was the RR of all-grade (G) and G3-5 infections for patients receiving ICI-based treatments. Random or fixed-effect models were used according to statistical heterogeneity.
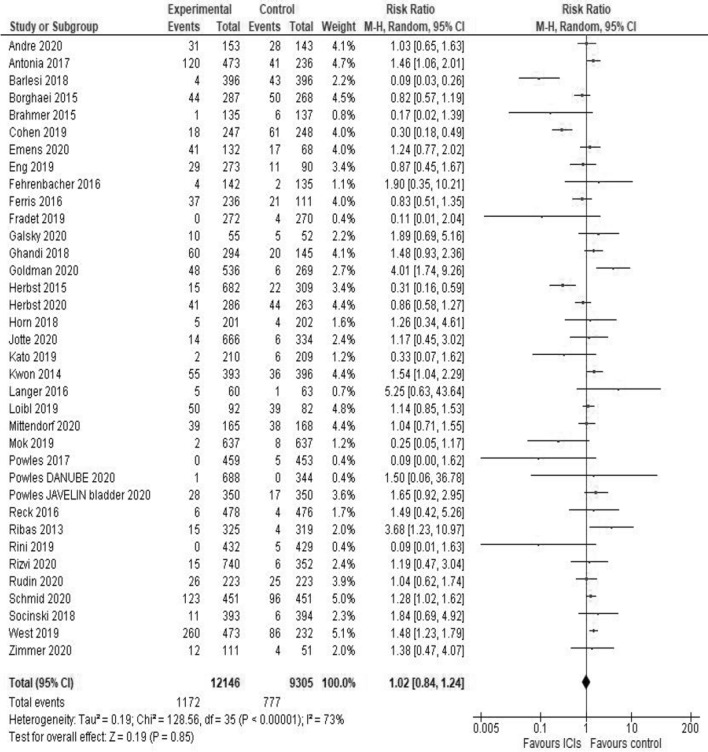
Results: A total of 21,451 patients from N = 36 studies were eligible. ICIs were associated with a similar risk of all-grade infections (RR = 1.02; 95% CI 0.84-1.24; P = 0.85) versus non-ICI treatments (G1-5 events: 9.6 versus 8.3%). When the ICIs alone were compared to CT, their use was associated with 42% less risk of all-grade infections (RR = 0.58, 95% CI 0.4-0.85; P = 0.01). Compared to CT, the combination of ICIs and CT increased the risk of all-grade (RR = 1.37, 95% CI 1.23-1.53; P < 0.01) and severe infections (RR = 1.52, 95% CI 1.17-1.96; P < 0.01). In anti-PD-1, anti-PD-L1, anti-CTLA-4, monotherapy, and combination trials, the RR of all-grade infections was 0.72 (95% CI 0.49-1.05; P = 0.09), 1.18 (95% CI 0.95-1.46; P = 0.13), 1.74 (95% CI 1.13-2.67; P = 0.01), 0.97 (95% CI 0.79-1.19; P = 0.75) and 2.26 (95% CI 1.34-3.8; P < 0.01), respectively.
Conclusions: Compared to CT alone, ICIs were safer and are recommended for frail patients. Conversely, CT + ICIs or ICIs combinations increased infection risk. Further studies are required to identify high-risk patients and evaluate the need for CT dose reduction or prophylactic myeloid growth factors.
© 2021. The Author(s), under exclusive licence to Springer Nature Switzerland AG.
Conflict of interest statement
Fausto Petrelli, Anna Maria Morelli, Andrea Luciani, Antonio Ghidini, and Cinzia Solinas declare that they have no conflicts of interest that might be relevant to the contents of this article.
Figures




References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
