

Immunogenicity of the BNT162b2 COVID-19 mRNA vaccine and early clinical outcomes in patients with haematological malignancies in Lithuania: a national prospective cohort study
- PMID: 34224668
- PMCID: PMC8253543
- DOI: 10.1016/S2352-3026(21)00169-1
Immunogenicity of the BNT162b2 COVID-19 mRNA vaccine and early clinical outcomes in patients with haematological malignancies in Lithuania: a national prospective cohort study
Abstract
Background: Haematological malignancies and their treatments are likely to affect SARS-CoV-2 vaccine efficacy. We aimed to evaluate serological response to BNT162b2 vaccine in patients with haematological malignancies by type of treatment.
Methods: Our national prospective cohort study was done in Lithuania and assessed serological response to one and two BNT162b2 (Comirnaty, Pfizer-BioNTech) vaccine doses in healthy health-care workers and in patients with haematological malignancies. Eligible participants were aged 18 years or older, had received both vaccine doses, and had available biobanked blood samples from before vaccination and after the second dose. Biobanked samples and health data were obtained from Vilnius University Hospital Santaros Klinikos Biobank. Abbott Architect SARS-CoV-2 IgG Quant II chemiluminescent microparticle assay was used to quantify serum anti-SARS-CoV-2-S1 IgG antibody (anti-S1 IgG antibody) concentrations 0-10 days before the first BNT162b2 vaccine, on the day of second immunisation (around day 21), and 7 to 21 days after the second immunisation. Adverse events were assessed by a standardised questionnaire. Breakthrough infections were characterised clinically and by SARS-CoV-2 genotyping whenever possible. This study is registered with ClinicalTrials.gov, NCT04871165.
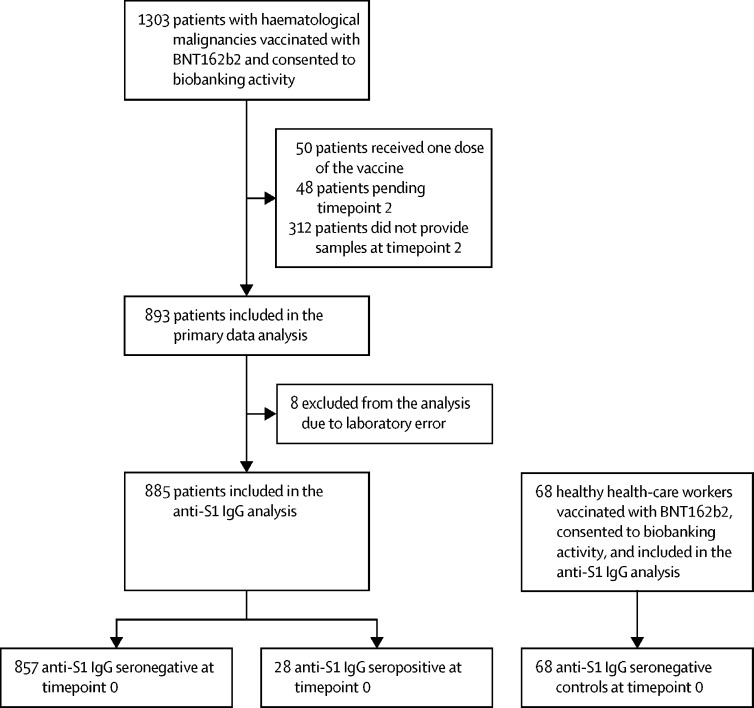
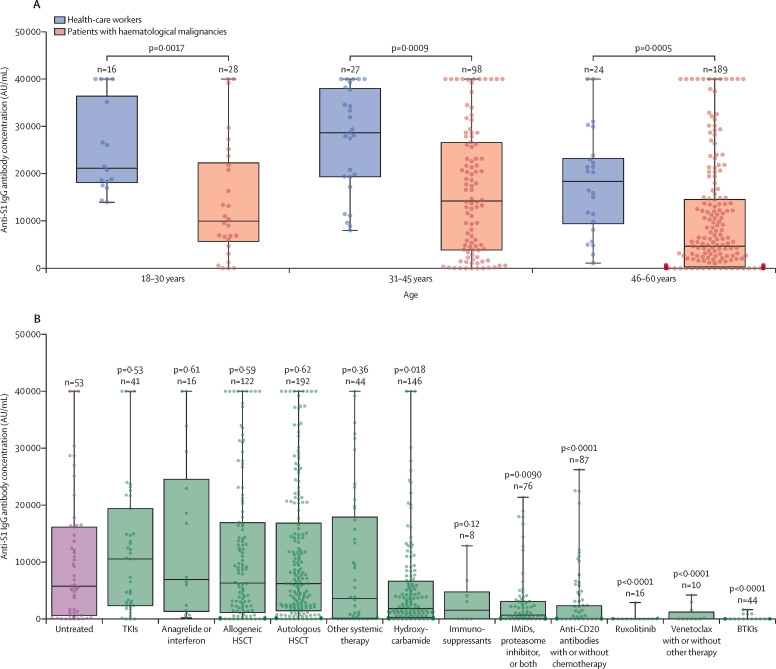
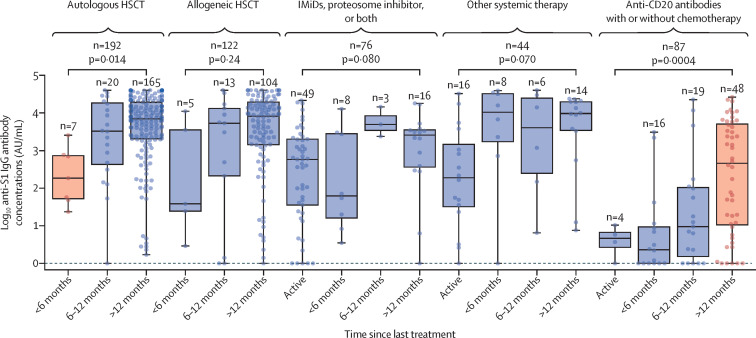
Findings: Between Jan 8 and April 21, 2021, 885 participants with haematological malignancies were included in the study. 857 patients were anti-S1 IgG seronegative at timepoint 0 and constituted the main analysis cohort. The age-matched comparison was made between 315 patients with haematological malignancies who were aged 18-60 years and 67 healthy health-care workers in the same age group. Patients aged 18-60 years with haematological malignancies had lower median anti-S1 IgG antibody responses after two BNT162b2 vaccine doses than did health-care workers of the same age group (median 6961 AU/mL [IQR 1292-20 672] vs 21 395 AU/mL [14 831-33 553]; p<0·0001). Compared with untreated patients with haematological malignancies (n=53; median 5761 AU/mL [629-16 141]), patients actively treated with Bruton tyrosine kinase inhibitors (BTKIs; n=44; 0 AU/mL [0-7]; p<0·0001), ruxolitinib (n=16; 10 AU/mL [0-45]; p<0·0001), venetoclax (n=10; 4 AU/mL [0-1218]; p=0·0005), or anti-CD20 antibody therapy (n=87; 17 AU/mL [1-2319]; p<0·0001) showed particularly poor anti-S1 IgG antibody responses following two BNT162b2 doses. Patients being treated with tyrosine kinase inhibitors (n=41; 10 537 AU/mL [IQR 2335-19 388]) or patients who received autologous haematopoietic stem-cell transplantation (HSCT; n=192; 6203 AU/mL [1451-16 834]) or allogeneic HSCT (n=122; 6304 AU/mL [1120-16 913]) were among the subgroups with the highest numerical responses. Nine SARS-CoV-2 infections and three COVID-19 deaths were observed among fully vaccinated patients with haematological malignancies.
Interpretation: Patients with haematological malignancies mount blunted and heterogeneous antibody responses to the full course of BNT162b2 mRNA vaccination. Patients who are actively treated with BTKIs, ruxolitinib, venetoclax, or anti-CD20 antibody therapies seem to be the most negatively affected and might be left unprotected from SARS-CoV-2 infection. Breakthrough severe SARS-CoV-2 infections in fully vaccinated patients with haematological malignancies emphasise the importance of ongoing strict adherence to non-pharmacological interventions and household vaccination while SARS-CoV-2 is circulating in the community.
Funding: Vilnius University Hospital Santaros Klinikos.
Translation: For the Lithuanian translation of the abstract see Supplementary Materials section.
Copyright © 2021 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests We declare no competing interests.
Figures
References
-
- Sahin U, Muik A, Derhovanessian E, et al. COVID-19 vaccine BNT162b1 elicits human antibody and TH1 T cell responses. Nature. 2020;586:594–599. - PubMed
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
