

Clinical characteristics and outcomes of invasively ventilated patients with COVID-19 in Argentina (SATICOVID): a prospective, multicentre cohort study
- PMID: 34224674
- PMCID: PMC8253540
- DOI: 10.1016/S2213-2600(21)00229-0
Clinical characteristics and outcomes of invasively ventilated patients with COVID-19 in Argentina (SATICOVID): a prospective, multicentre cohort study
Abstract
Background: Although COVID-19 has greatly affected many low-income and middle-income countries, detailed information about patients admitted to the intensive care unit (ICU) is still scarce. Our aim was to examine ventilation characteristics and outcomes in invasively ventilated patients with COVID-19 in Argentina, an upper middle-income country.
Methods: In this prospective, multicentre cohort study (SATICOVID), we enrolled patients aged 18 years or older with RT-PCR-confirmed COVID-19 who were on invasive mechanical ventilation and admitted to one of 63 ICUs in Argentina. Patient demographics and clinical, laboratory, and general management variables were collected on day 1 (ICU admission); physiological respiratory and ventilation variables were collected on days 1, 3, and 7. The primary outcome was all-cause in-hospital mortality. All patients were followed until death in hospital or hospital discharge, whichever occurred first. Secondary outcomes were ICU mortality, identification of independent predictors of mortality, duration of invasive mechanical ventilation, and patterns of change in physiological respiratory and mechanical ventilation variables. The study is registered with ClinicalTrials.gov, NCT04611269, and is complete.
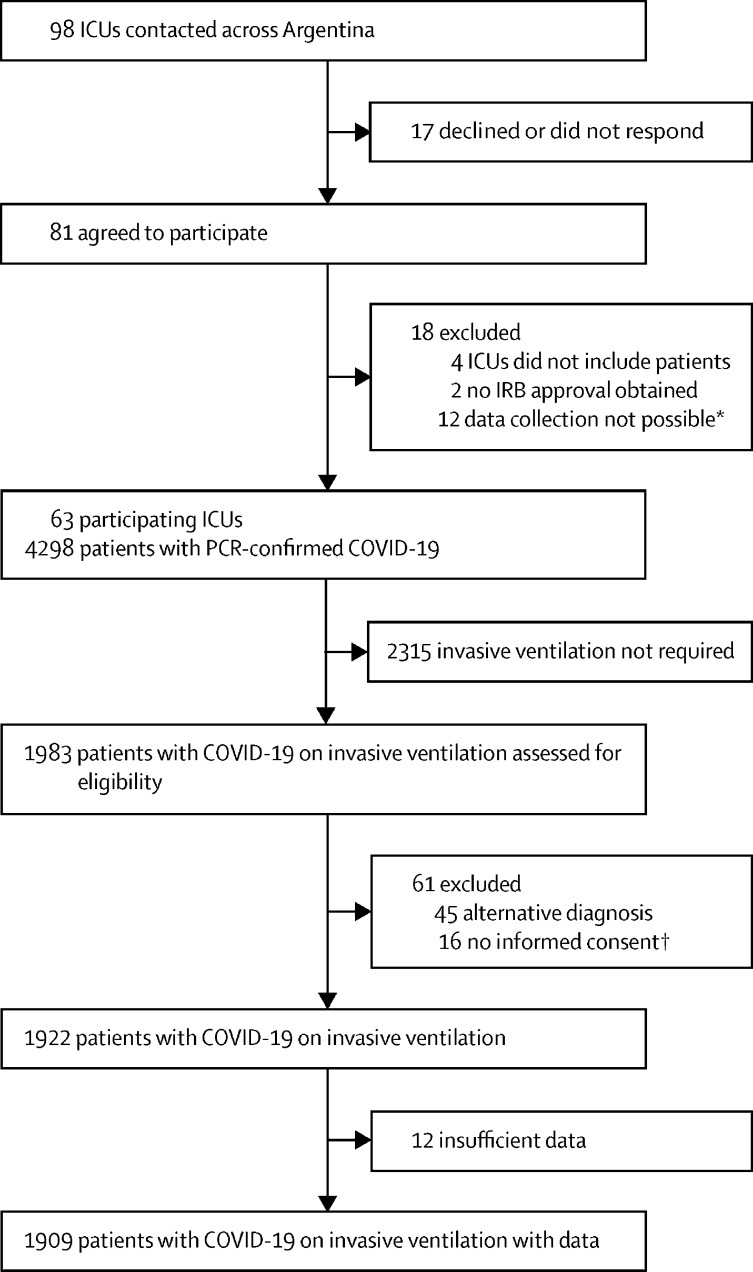
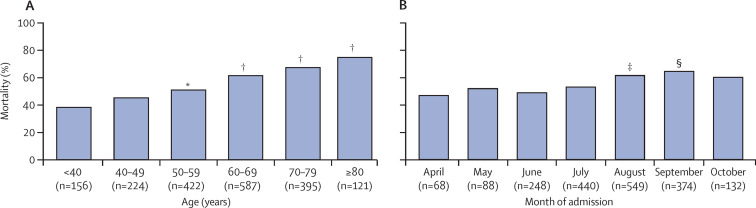
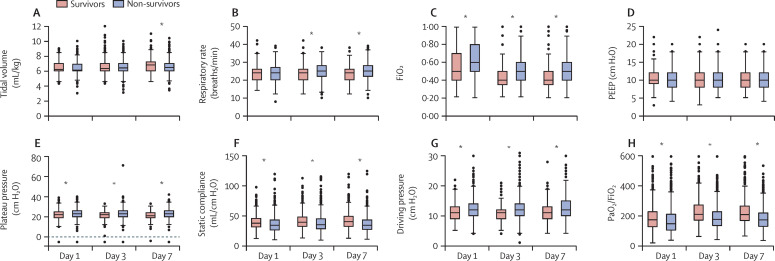
Findings: Between March 20, 2020, and Oct 31, 2020, we enrolled 1909 invasively ventilated patients with COVID-19, with a median age of 62 years [IQR 52-70]. 1294 (67·8%) were men, hypertension and obesity were the main comorbidities, and 939 (49·2%) patients required vasopressors. Lung-protective ventilation was widely used and median duration of ventilation was 13 days (IQR 7-22). Median tidal volume was 6·1 mL/kg predicted bodyweight (IQR 6·0-7·0) on day 1, and the value increased significantly up to day 7; positive end-expiratory pressure was 10 cm H2O (8-12) on day 1, with a slight but significant decrease to day 7. Ratio of partial pressure of arterial oxygen (PaO2) to fractional inspired oxygen (FiO2) was 160 (IQR 111-218), respiratory system compliance 36 mL/cm H2O (29-44), driving pressure 12 cm H2O (10-14), and FiO2 0·60 (0·45-0·80) on day 1. Acute respiratory distress syndrome developed in 1672 (87·6%) of patients; 1176 (61·6%) received prone positioning. In-hospital mortality was 57·7% (1101/1909 patients) and ICU mortality was 57·0% (1088/1909 patients); 462 (43·8%) patients died of refractory hypoxaemia, frequently overlapping with septic shock (n=174). Cox regression identified age (hazard ratio 1·02 [95% CI 1·01-1·03]), Charlson score (1·16 [1·11-1·23]), endotracheal intubation outside of the ICU (ie, before ICU admission; 1·37 [1·10-1·71]), vasopressor use on day 1 (1·29 [1·07-1·55]), D-dimer concentration (1·02 [1·01-1·03]), PaO2/FiO2 on day 1 (0·998 [0·997-0·999]), arterial pH on day 1 (1·01 [1·00-1·01]), driving pressure on day 1 (1·05 [1·03-1·08]), acute kidney injury (1·66 [1·36-2·03]), and month of admission (1·10 [1·03-1·18]) as independent predictors of mortality.
Interpretation: In patients with COVID-19 who required invasive mechanical ventilation, lung-protective ventilation was widely used but mortality was high. Predictors of mortality in our study broadly agreed with those identified in studies of invasively ventilated patients in high-income countries. The sustained burden of COVID-19 on scarce health-care personnel might have contributed to high mortality over the course of our study in Argentina. These data might help to identify points for improvement in the management of patients in middle-income countries and elsewhere.
Funding: None.
Translation: For the Spanish translation of the Summary see Supplementary Materials section.
Copyright © 2021 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests The authors declare no competing interests.
Figures
Comment in
-
Elisa Estenssoro: a career devoted to critical care.Lancet Respir Med. 2021 Sep;9(9):951-952. doi: 10.1016/S2213-2600(21)00321-0. Epub 2021 Jul 2. Lancet Respir Med. 2021. PMID: 34224672 Free PMC article. No abstract available.
References
-
- WHO WHO coronavirus disease (COVID-19) dashboard. https://covid19.who.int/
-
- The Lancet COVID-19 in Latin America: a humanitarian crisis. Lancet. 2020;396 - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
