

Cardiac involvement in consecutive unselected hospitalized COVID-19 population: In-hospital evaluation and one-year follow-up
- PMID: 34224766
- PMCID: PMC8253670
- DOI: 10.1016/j.ijcard.2021.06.056
Cardiac involvement in consecutive unselected hospitalized COVID-19 population: In-hospital evaluation and one-year follow-up
Abstract
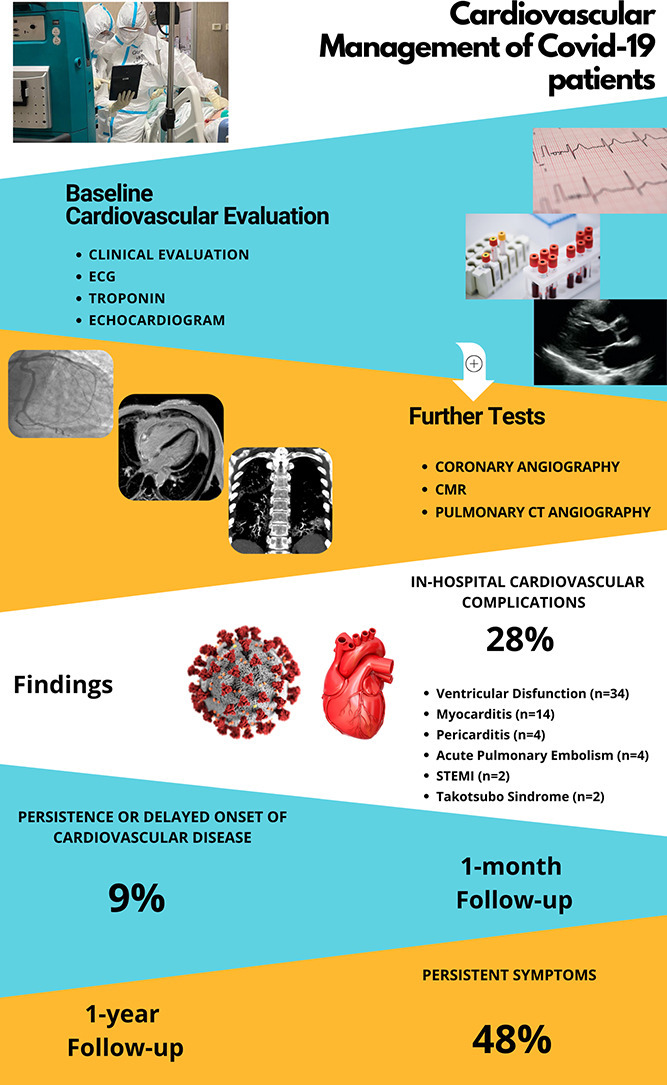
Background: Cardiovascular disease (CVD) can occur in COVID-19 and has impact on clinical course. Data on CVD prevalence in hospitalized COVID-19 patients and sequelae in survivors is limited. Aim of this prospective study carried out on consecutive unselected COVID-19 population, was to assess: 1) CVD occurrence among hospitalized COVID-19 patients, 2) persistence or new onset of CVD at one-month and one-year follow-up.
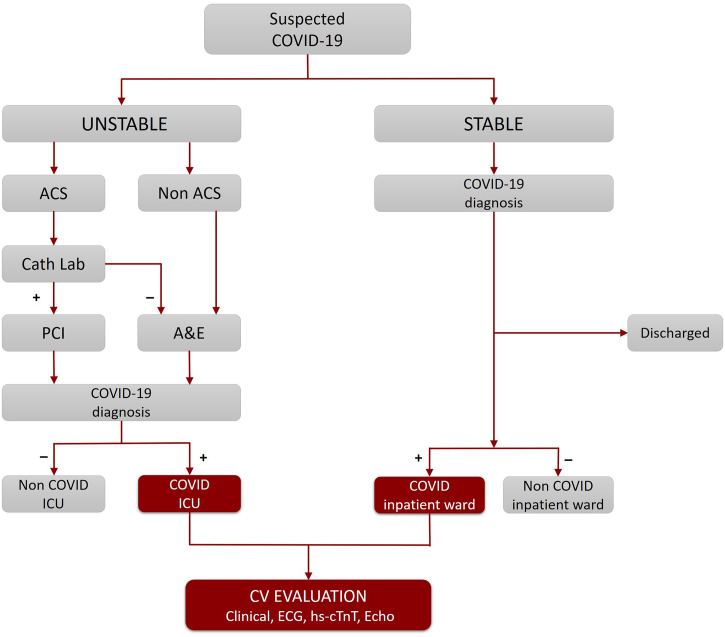
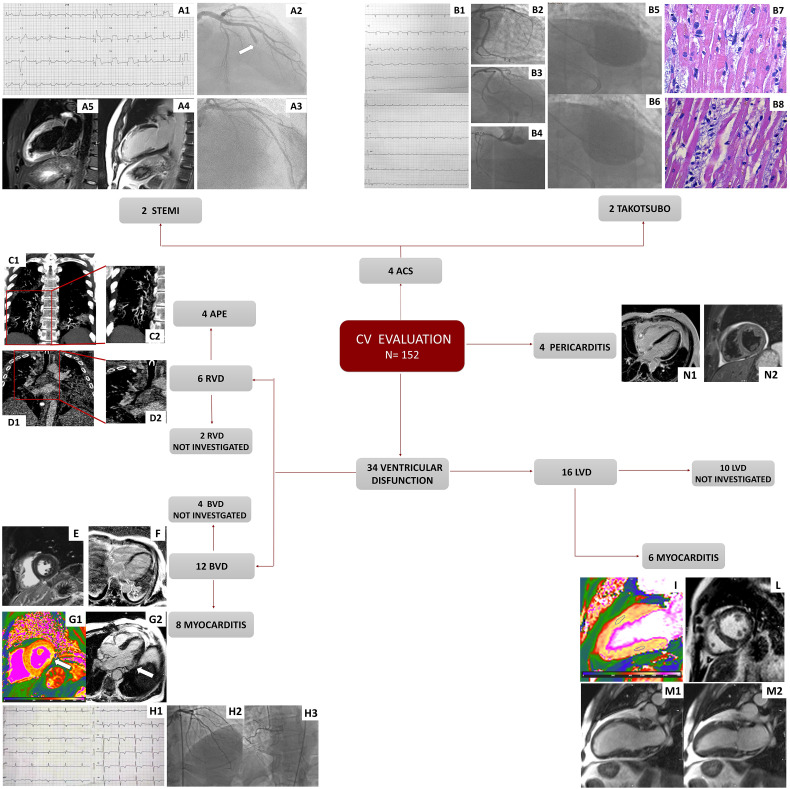
Methods: Over 30 days n = 152 COVID-19 patients underwent cardiovascular evaluation. Standard electrocardiogram (ECG), Troponin and echocardiography were integrated by further tests when indicated. Medical history, arterial blood gas, blood tests, chest computed tomography and treatment were recorded. CVD was defined as the occurrence of a new condition during the hospitalization for COVID-19. Survivors attended a one-month follow-up visit and a one-year telephone follow-up.
Results: Forty-two patients (28%) experienced a wide spectrum of CVD with acute myocarditis being the most frequent. Death occurred in 32 patients (21%) and more frequently in patients who developed CVD (p = 0.032). After adjustment for confounders, CVD was independently associated with death occurrence. At one-month follow-up visit, 7 patients (9%) presented persistent or delayed CVD. At one-year telephone follow-up, 57 patients (48%) reported persistent symptoms.
Conclusion: Cardiovascular evaluation in COVID-19 patients is crucial since the occurrence of CVD in hospitalized COVID-19 patients is common (28%), requires specific treatment and increases the risk of in-hospital mortality. Persistence or delayed presentation of CVD at 1-month (9%) and persistent symptoms at 1-year follow-up (48%) suggest the need for monitoring COVID-19 survivors.
Keywords: COVID-19; Cardiovascular disease; Cardiovascular magnetic resonance; Echocardiography; Follow-up; Myocarditis.
Copyright © 2021. Published by Elsevier B.V.
Conflict of interest statement
The authors report no relationships that could be construed as a conflict of interest.
Figures
Comment in
-
Multimodality evaluation of cardiac injury in COVID-19: Getting to the heart of the matter.Int J Cardiol. 2021 Sep 15;339:243-245. doi: 10.1016/j.ijcard.2021.07.031. Epub 2021 Jul 21. Int J Cardiol. 2021. PMID: 34298070 Free PMC article. No abstract available.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
