

Use of cast immobilisation versus removable brace in adults with an ankle fracture: multicentre randomised controlled trial
- PMID: 34226192
- PMCID: PMC8256800
- DOI: 10.1136/bmj.n1506
Use of cast immobilisation versus removable brace in adults with an ankle fracture: multicentre randomised controlled trial
Abstract
Objectives: To assess function, quality of life, resource use, and complications in adults treated with plaster cast immobilisation versus a removable brace for ankle fracture.
Design: Multicentre randomised controlled trial.
Setting: 20 trauma units in the UK National Health Service.
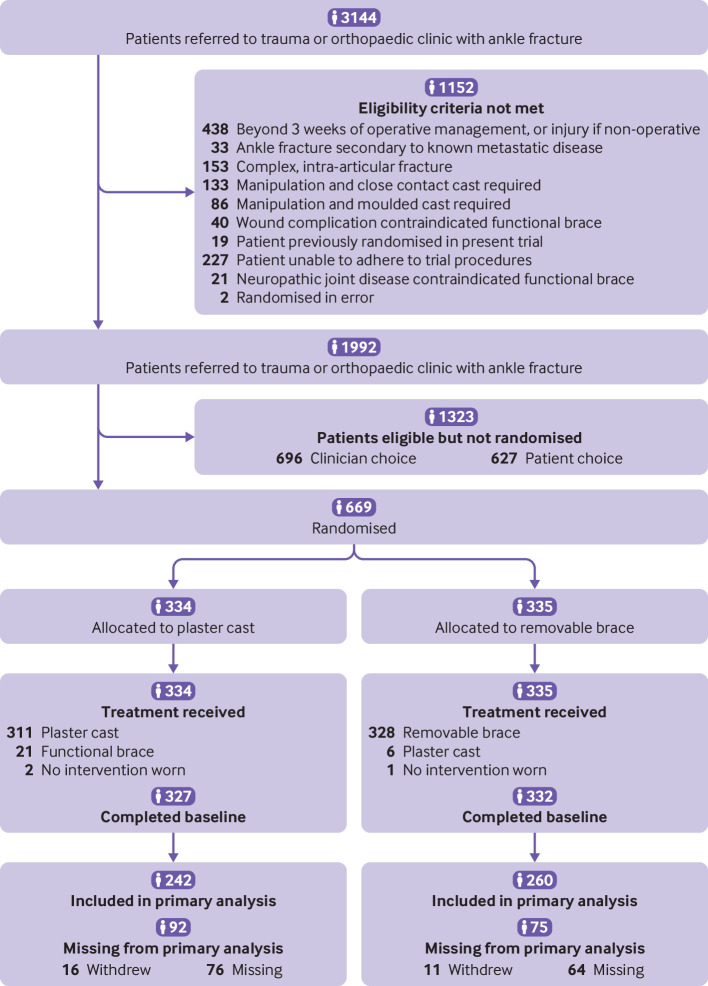
Participants: 669 adults aged 18 years and older with an acute ankle fracture suitable for cast immobilisation: 334 were randomised to a plaster cast and 335 to a removable brace.
Interventions: A below the knee cast was applied and ankle range of movement exercises started on cast removal. The removable brace was fitted, and ankle range of movement exercises were started immediately.
Main outcome measures: Primary outcome was the Olerud Molander ankle score at 16 weeks, analysed by intention to treat. Secondary outcomes were Manchester-Oxford foot questionnaire, disability rating index, quality of life, and complications at 6, 10, and 16 weeks.
Results: The mean age of participants was 46 years (SD 17 years) and 381 (57%) were women. 502 (75%) participants completed the study. No statistically significant difference was found in the Olerud Molander ankle score between the cast and removable brace groups at 16 weeks (favours brace: 1.8, 95% confidence interval -2.0 to 5.6). No clinically significant differences were found in the Olerud Molander ankle scores at other time points, in the secondary unadjusted, imputed, or per protocol analyses.
Conclusions: Traditional plaster casting was not found to be superior to functional bracing in adults with an ankle fracture. No statistically difference was found in the Olerud Molander ankle score between the trial arms at 16 weeks.
Trial registration: ISRCTN registry ISRCTN15537280.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: all authors had financial support from the National Institute for Health Research (NIHR) for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years. RSK is a member of the UK NIHR Health Technology Assessment (HTA) Cost Effectiveness Threshold (CET) board, NIHR Integrated Clinical Academic (ICA) doctoral panel, and chair of the NIHR Research for Patient Benefit (RfPB) board. MLC is a member of the UK NIHR HTA general board and holder of a NIHR senior investigator award. ACR is a member of the NIHR ICA clinical lectureship/senior clinical lectureship panel and holder of a NIHR senior investigator award. RSK, MLC, ACR, NP, HP, and PW have been awarded current and previous NIHR research grants. HP, MU, and RSK are co-investigators on two NIHR funded studies receiving additional support from Stryker. MU is chief investigator or co-investigator on multiple previous and current research grants from the UK NIHR and Arthritis Research UK and is a co-investigator on grants funded by the Australian National Health and Medical Research Council. He is an NIHR senior investigator. He has received travel expenses for speaking at conferences from the professional organisations hosting the conferences. He is a director and shareholder of Clinvivo that provides electronic data collection for health services research. He is part of an academic partnership with Serco, funded by the European Social Fund, related to return to work initiatives. He has accepted honorariums for teaching and lecturing from consortium for advanced research training in Africa. Until March 2020 he was an editor of the NIHR journal series and a member of the NIHR Journal Editors Group, for which he received a fee.
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous