

Socio-economic position as a moderator of cardiometabolic outcomes in patients receiving psychotropic treatment associated with weight gain: results from a prospective 12-month inception cohort study and a large population-based cohort
- PMID: 34226496
- PMCID: PMC8257637
- DOI: 10.1038/s41398-021-01482-9
Socio-economic position as a moderator of cardiometabolic outcomes in patients receiving psychotropic treatment associated with weight gain: results from a prospective 12-month inception cohort study and a large population-based cohort
Erratum in
-
Correction: Socio-economic position as a moderator of cardiometabolic outcomes in patients receiving psychotropic treatment associated with weight gain: results from a prospective 12-month inception cohort study and a large population-based cohort.Transl Psychiatry. 2021 Oct 7;11(1):512. doi: 10.1038/s41398-021-01520-6. Transl Psychiatry. 2021. PMID: 34620835 Free PMC article. No abstract available.
Abstract
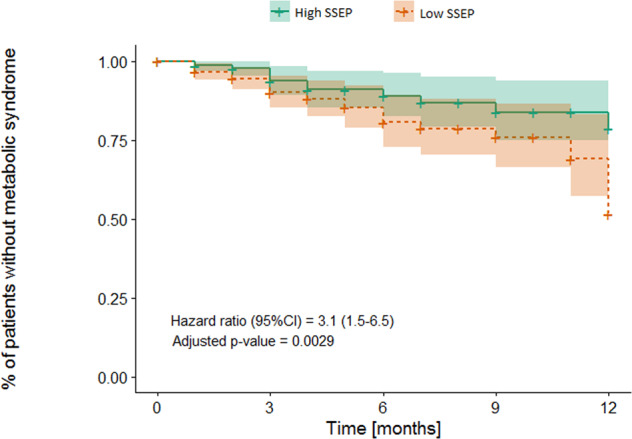
Weight gain and metabolic complications are major adverse effects of many psychotropic drugs. We aimed to understand how socio-economic status (SES), defined as the Swiss socio-economic position (SSEP), is associated with cardiometabolic parameters after initiation of psychotropic medications known to induce weight gain. Cardiometabolic parameters were collected in two Swiss cohorts following the prescription of psychotropic medications. The SSEP integrated neighborhood-based income, education, occupation, and housing condition. The results were then validated in an independent replication sample (UKBiobank), using educational attainment (EA) as a proxy for SES. Adult patients with a low SSEP had a higher risk of developing metabolic syndrome over one year versus patients with a high SSEP (Hazard ratio (95% CI) = 3.1 (1.5-6.5), n = 366). During the first 6 months of follow-up, a significant negative association between SSEP and body mass index (BMI), weight change, and waist circumference change was observed (25 ≤ age < 65, n = 526), which was particularly important in adults receiving medications with the highest risk of weight gain, with a BMI difference of 0.86 kg/m2 between patients with low versus high SSEP (95% CI: 0.03-1.70, n = 99). Eventually, a causal effect of EA on BMI was revealed using Mendelian randomization in the UKBiobank, which was notably strong in high-risk medication users (beta: -0.47 SD EA per 1 SD BMI; 95% CI: -0.46 to -0.27, n = 11,314). An additional aspect of personalized medicine was highlighted, suggesting the patients' SES represents a significant risk factor. Particular attention should be paid to patients with low SES when initiating high cardiometabolic risk psychotropic medications.
Conflict of interest statement
CE received honoraria for conferences or teaching CME courses from Janssen-Cilag, Lundbeck, Otsuka, Sandoz, Servier, Sunovion, Vifor-Pharma, and Zeller in the past 3 years. AvG received honoraria for a conference or workshop participation from Vifor and Schwabe in the previous 3 years. Dr. Correll has been a consultant and/or advisor to or has received honoraria from: Alkermes, Allergan, Angelini, Gedeon Richter, Gerson Lehrman Group, IntraCellular Therapies, Janssen/J&J, LB Pharma, Lundbeck, MedAvante-ProPhase, Medscape, Neurocrine, Noven, Otsuka, Pfizer, Recordati, Rovi, Sumitomo Dainippon, Sunovion, Supernus, Takeda, and Teva. He has provided expert testimony for Janssen and Otsuka. He served on a Data Safety Monitoring Board for Lundbeck, Rovi, Supernus, and Teva. He received royalties from UpToDate and grant support from Janssen and Takeda. He is also a stock option holder of LB Pharma. The other authors declare no competing interests.
Figures
References
-
- Correll CU, Solmi M, Veronese N, Bortolato B, Rosson S, Santonastaso P, et al. Prevalence, incidence and mortality from cardiovascular disease in patients with pooled and specific severe mental illness: a large-scale meta-analysis of 3,211,768 patients and 113,383,368 controls. World Psychiatry. 2017;16:163–80. doi: 10.1002/wps.20420. - DOI - PMC - PubMed
