

Pathophysiology of COVID-19-associated acute kidney injury
- PMID: 34226718
- PMCID: PMC8256398
- DOI: 10.1038/s41581-021-00452-0
Pathophysiology of COVID-19-associated acute kidney injury
Abstract
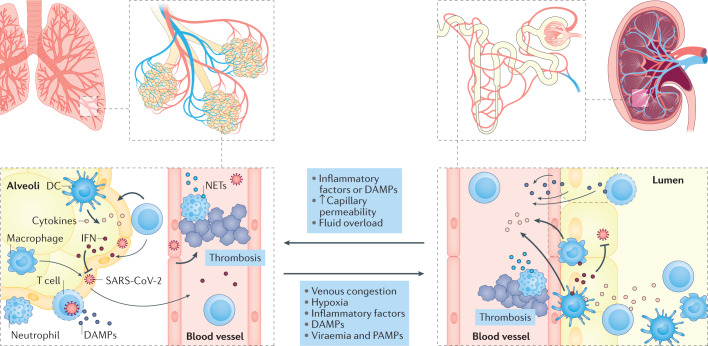
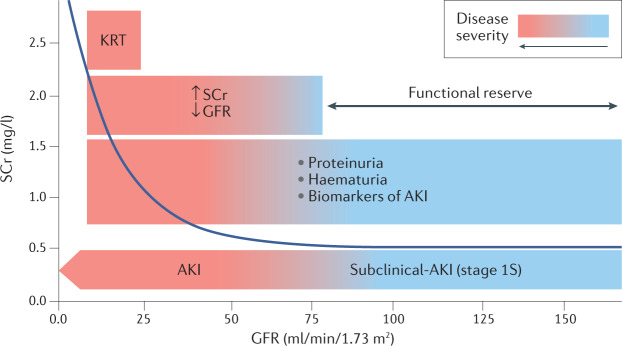
Although respiratory failure and hypoxaemia are the main manifestations of COVID-19, kidney involvement is also common. Available evidence supports a number of potential pathophysiological pathways through which acute kidney injury (AKI) can develop in the context of SARS-CoV-2 infection. Histopathological findings have highlighted both similarities and differences between AKI in patients with COVID-19 and in those with AKI in non-COVID-related sepsis. Acute tubular injury is common, although it is often mild, despite markedly reduced kidney function. Systemic haemodynamic instability very likely contributes to tubular injury. Despite descriptions of COVID-19 as a cytokine storm syndrome, levels of circulating cytokines are often lower in patients with COVID-19 than in patients with acute respiratory distress syndrome with causes other than COVID-19. Tissue inflammation and local immune cell infiltration have been repeatedly observed and might have a critical role in kidney injury, as might endothelial injury and microvascular thrombi. Findings of high viral load in patients who have died with AKI suggest a contribution of viral invasion in the kidneys, although the issue of renal tropism remains controversial. An impaired type I interferon response has also been reported in patients with severe COVID-19. In light of these observations, the potential pathophysiological mechanisms of COVID-19-associated AKI may provide insights into therapeutic strategies.
© 2021. Springer Nature Limited.
Conflict of interest statement
The authors declare no competing interests.
Figures
Comment in
-
Antineutrophil cytoplasmic autoantibody-associated vasculitis with rapid progressive glomerulonephritis following SARS-CoV-2 infection: a cause or coincidence?Pol Arch Intern Med. 2022 Mar 30;132(3):16165. doi: 10.20452/pamw.16165. Epub 2021 Dec 8. Pol Arch Intern Med. 2022. PMID: 34878237 No abstract available.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
