

Bacterial coinfection among coronavirus disease 2019 patient groups: an updated systematic review and meta-analysis
- PMID: 34226847
- PMCID: PMC8245302
- DOI: 10.1016/j.nmni.2021.100910
Bacterial coinfection among coronavirus disease 2019 patient groups: an updated systematic review and meta-analysis
Abstract
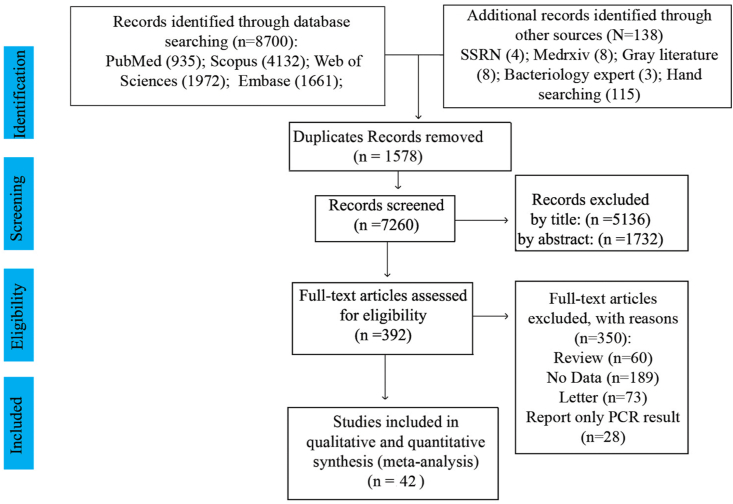
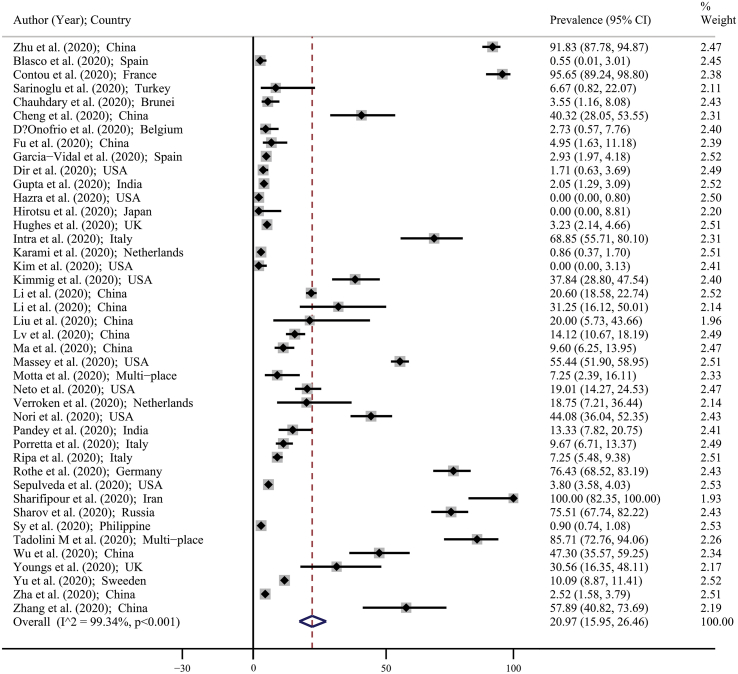
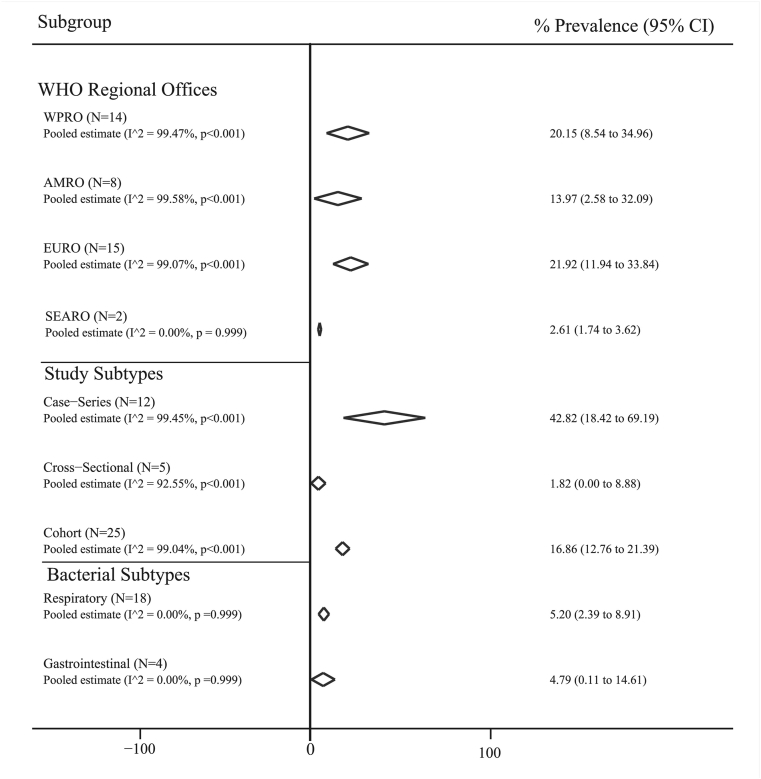
The pandemic of severe acute respiratory syndrome coronavirus 2 raised the attention towards bacterial coinfection and its role in coronavirus disease 2019 (COVID-19) disease. This study aims to systematically review and identify the pooled prevalence of bacterial coinfection in the related articles. A comprehensive search was conducted in international databases, including MEDLINE, Scopus, Web of Science, and Embase, to identify the articles on the prevalence of bacterial coinfections in COIVD-19 patients from 1 December 2019 until 30 December 2020. All observational epidemiological studies that evaluated the prevalence of bacterial coinfections in patients with COVID-19 were included without any restriction. Forty-two studies including a total sample size of 54,695 were included in the analysis. The pooled estimate for the prevalence of bacterial coinfections was 20.97% (95% CI: 15.95-26.46), and the pooled prevalence of bacterial coinfections was 5.20% (95% CI: 2.39-8.91) for respiratory subtype and 4.79% (95% CI: 0.11-14.61) for the gastrointestinal subtype. The pooled prevalence for Eastern Mediterranean Regional Office and South-East Asia Regional Office was 100% (95% CI: 82.35-100.00) and 2.61% (95% CI: 1.74-3.62). This rate of coinfection poses a great danger towards patients, especially those in critical condition. Although there are multiple complications and adverse effects related to extensive use of antibiotics to treat patients with COVID-19, it seems there is no other option except applying them, and it needs to be done carefully.
Keywords: COVID-19; Coinfection; coronavirus; meta-analysis; systematics review.
© 2021 The Authors.
Figures
References
-
- Kumar A., Zarychanski R., Pinto R., Cook D.J., Marshall J., Lacroix J. Critically ill patients with 2009 influenza A (H1N1) infection in Canada. Jama. 2009;302(17):1872–1879. - PubMed
-
- Beadling C., Slifka M.K. How do viral infections predispose patients to bacterial infections? Curr Opin Infect Dise. 2004;17(3):185–191. - PubMed
LinkOut - more resources
Full Text Sources