

Multicenter Study
doi: 10.1093/bjs/znab183.
Machine learning risk prediction of mortality for patients undergoing surgery with perioperative SARS-CoV-2: the COVIDSurg mortality score
Collaborators
- PMID: 34227657
- PMCID: PMC8344569
- DOI: 10.1093/bjs/znab183
Item in Clipboard
Multicenter Study
Machine learning risk prediction of mortality for patients undergoing surgery with perioperative SARS-CoV-2: the COVIDSurg mortality score
Br J Surg.
.
Abstract
To support the global restart of elective surgery, data from an international prospective cohort study of 8492 patients (69 countries) was analysed using artificial intelligence (machine learning techniques) to develop a predictive score for mortality in surgical patients with SARS-CoV-2. We found that patient rather than operation factors were the best predictors and used these to create the COVIDsurg Mortality Score (
Figures
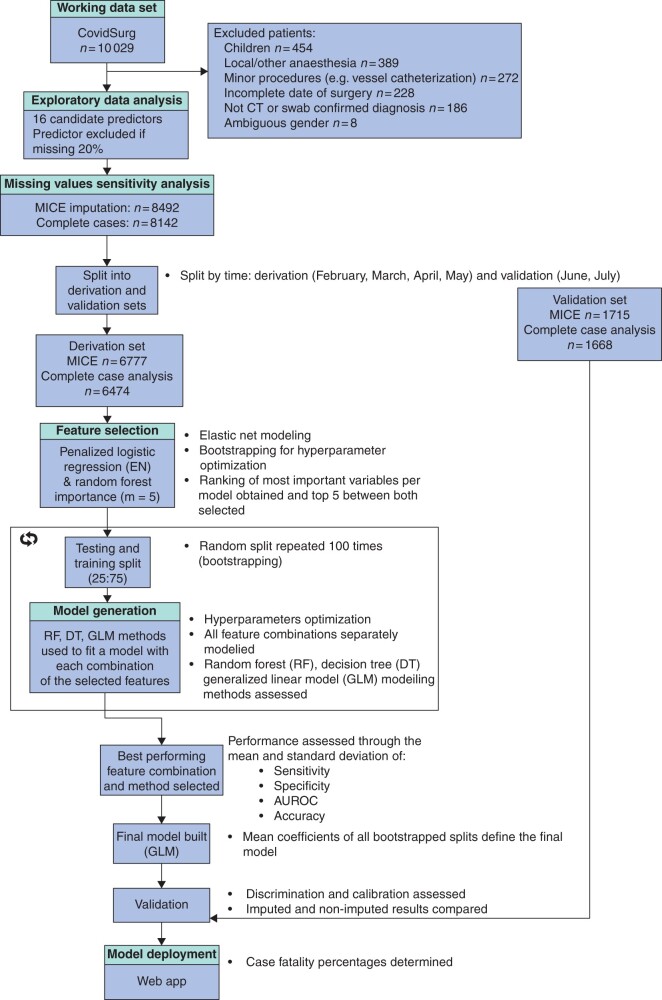
Cohort study patient inclusion and model derivation and validation flow MICE, multiple imputation by chained equations; EN, elastic net.
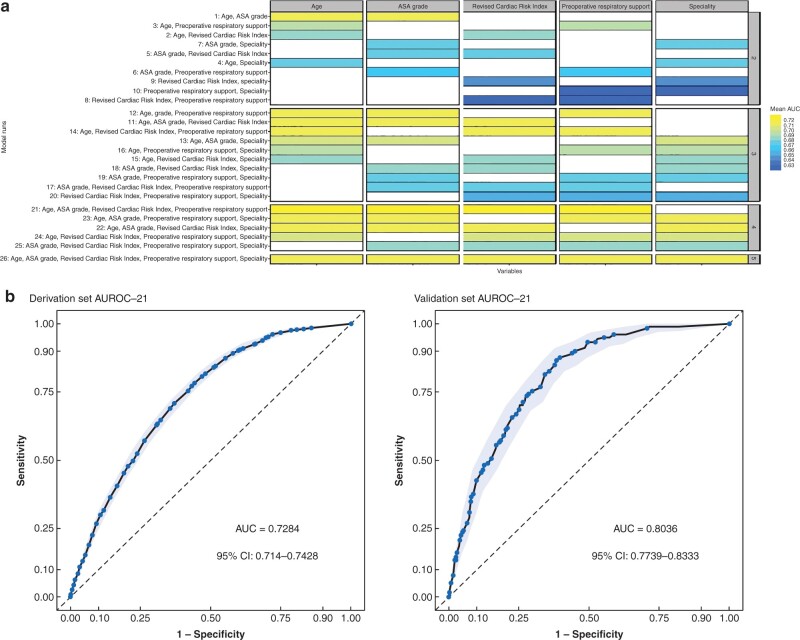
Model performance and evaluation. a Logistic model performance of all different runs divided by each of the features. Colour coded according to performance values (mean area under the curve (AUC) of 100 bootstraps). b Receiver operating characteristic curves for model evaluation. After generating the final model made up by the averaged coefficients of the bootstraps of run 21, it was evaluated in both the derivation set as a whole (Area under receiver operating characteristic curve (AUROC) = 0.7284, 95 per cent c.i. 0.7140 to 0.7428) and the validation set AUROC = 0.8036, 95 per cent c.i. 0.7739 to 0.8333). Results are depicted with AUROC and confidence intervals generated through the pROC and plotROC packages. 95 per cent confidence intervals were computed with default 2000 stratified bootstrap replicates.
References
-
- Kibbe MR. Surgery and COVID-19. JAMA 2020;324:1151–1152. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
- Archivio Istituzionale della Ricerca Unimi - Access Free Full Text
- Europe PubMed Central
- Linkoping University Electronic Press
- ORBi (University of Liege)
- Ovid Technologies, Inc.
- PubMed Central
- Silverchair Information Systems
- White Rose Research Online
- eScholarship, University of California - Access Free Full Text
Medical
Miscellaneous
