

Is Anterior Rotation of the Acetabulum Necessary to Normalize Joint Contact Pressure in Periacetabular Osteotomy? A Finite-element Analysis Study
- PMID: 34228657
- PMCID: PMC8673984
- DOI: 10.1097/CORR.0000000000001893
Is Anterior Rotation of the Acetabulum Necessary to Normalize Joint Contact Pressure in Periacetabular Osteotomy? A Finite-element Analysis Study
Abstract
Background: Inappropriate sagittal plane correction can result in an increased risk of osteoarthritis progression after periacetabular osteotomy (PAO). Individual and postural variations in sagittal pelvic tilt, along with acetabular deformity, affect joint contact mechanics in dysplastic hips and may impact the direction and degree of acetabular correction. Finite-element analyses that account for physiologic pelvic tilt may provide valuable insight into the effect of PAO on the contact mechanics of dysplastic hips, which may lead to improved acetabular correction during PAO.
Questions/purposes: We performed virtual PAO using finite-element models with reference to the standing pelvic position to clarify (1) whether lateral rotation of the acetabulum normalizes the joint contact pressure, (2) risk factors for abnormal contact pressure after lateral rotation of the acetabulum, and (3) whether additional anterior rotation of the acetabulum further reduces contact pressure.
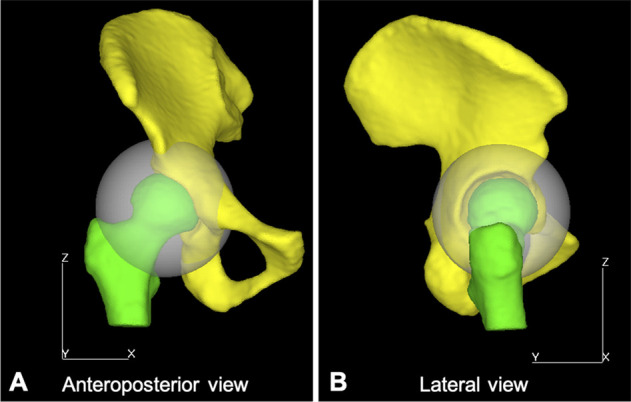
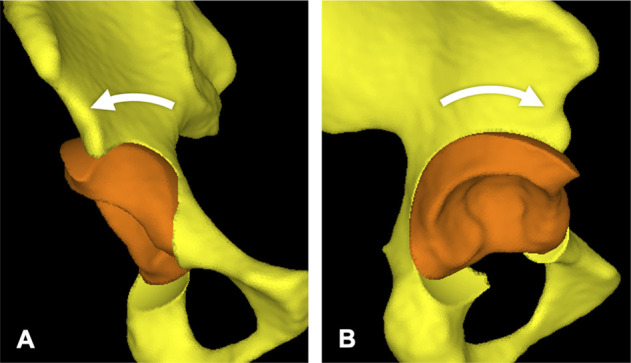
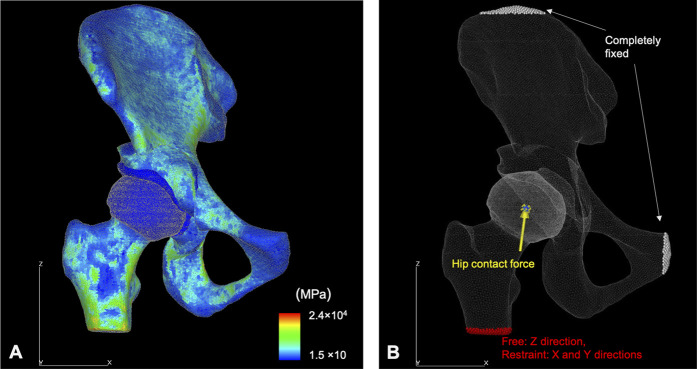
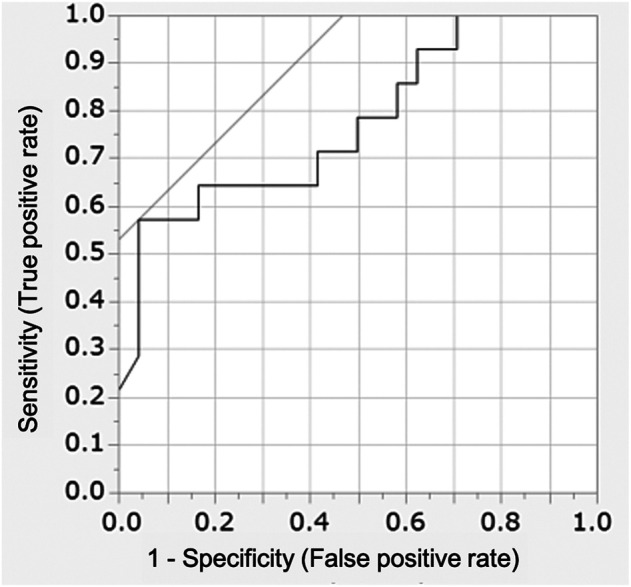
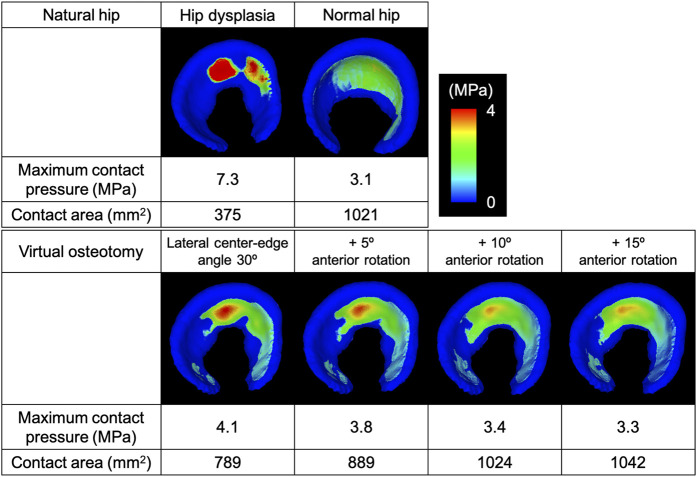
Methods: Between 2016 and 2020, 85 patients (92 hips) underwent PAO to treat hip dysplasia. Eighty-two patients with hip dysplasia (lateral center-edge angle < 20°) were included. Patients with advanced osteoarthritis, femoral head deformity, prior hip or spine surgery, or poor-quality images were excluded. Thirty-eight patients (38 hips) were eligible to participate in this study. All patients were women, with a mean age of 39 ± 10 years. Thirty-three women volunteers without a history of hip disease were reviewed as control participants. Individuals with a lateral center-edge angle < 25° or poor-quality images were excluded. Sixteen individuals (16 hips) with a mean age of 36 ± 7 years were eligible as controls. Using CT images, we developed patient-specific three-dimensional surface hip models with the standing pelvic position as a reference. The loading scenario was based on single-leg stance. Four patterns of virtual PAO were performed in the models. First, the acetabular fragment was rotated laterally in the coronal plane so that the lateral center-edge angle was 30°; then, anterior rotation in the sagittal plane was added by 0°, 5°, 10°, and 15°. We developed finite-element models for each acetabular position and performed a nonlinear contact analysis to calculate the joint contact pressure of the acetabular cartilage. The normal range of the maximum joint contact pressure was calculated to be < 4.1 MPa using a receiver operating characteristic curve. A paired t-test or Wilcoxon signed rank test with Bonferroni correction was used to compare joint contact pressures among acetabular positions. We evaluated the association of joint contact pressure with the patient-specific sagittal pelvic tilt and acetabular version and coverage using Pearson or Spearman correlation coefficients. An exploratory univariate logistic regression analysis was performed to identify which of the preoperative factors (CT measurement parameters and sagittal pelvic tilt) were associated with abnormal contact pressure after lateral rotation of the acetabulum. Variables with p values < 0.05 (anterior center-edge angle and sagittal pelvic tilt) were included in a multivariable model to identify the independent influence of each factor.
Results: Lateral rotation of the acetabulum decreased the median maximum contact pressure compared with that before virtual PAO (3.7 MPa [range 2.2-6.7] versus 7.2 MPa [range 4.1-14 MPa], difference of medians 3.5 MPa; p < 0.001). The resulting maximum contact pressures were within the normal range (< 4.1 MPa) in 63% of the hips (24 of 38 hips). The maximum contact pressure after lateral acetabular rotation was negatively correlated with the standing pelvic tilt (anterior pelvic plane angle) (ρ = -0.52; p < 0.001) and anterior center-edge angle (ρ = -0.47; p = 0.003). After controlling for confounding variables such as the lateral center-edge angle and sagittal pelvic tilt, we found that a decreased preoperative anterior center-edge angle (per 1°; odds ratio 1.14 [95% CI 1.01-1.28]; p = 0.01) was independently associated with elevated contact pressure (≥ 4.1 MPa) after lateral rotation; a preoperative anterior center-edge angle < 32° in the standing pelvic position was associated with elevated contact pressure (sensitivity 57%, specificity 96%, area under the curve 0.77). Additional anterior rotation further decreased the joint contact pressure; the maximum contact pressures were within the normal range in 74% (28 of 38 hips), 76% (29 of 38 hips), and 84% (32 of 38 hips) of the hips when the acetabulum was rotated anteriorly by 5°, 10°, and 15°, respectively.
Conclusion: Via virtual PAO, normal joint contact pressure was achieved in 63% of patients by normalizing the lateral acetabular coverage. However, lateral acetabular rotation was insufficient to normalize the joint contact pressure in patients with more posteriorly tilted pelvises and anterior acetabular deficiency. In patients with a preoperative anterior center-edge angle < 32° in the standing pelvic position, additional anterior rotation is expected to be a useful guide to normalize the joint contact pressure.
Clinical relevance: This virtual PAO study suggests that biomechanics-based planning for PAO should incorporate not only the morphology of the hip but also the physiologic pelvic tilt in the weightbearing position in order to customize acetabular reorientation for each patient.
Copyright © 2021 by the Association of Bone and Joint Surgeons.
Conflict of interest statement
Each author certifies that there are no funding or commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article related to the author or any immediate family members. All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research® editors and board members are on file with the publication and can be viewed on request.
Figures
Comment in
-
CORR Insights®: Is Anterior Rotation of the Acetabulum Necessary to Normalize Joint Contact Pressure in Periacetabular Osteotomy? A Finite-element Analysis Study.Clin Orthop Relat Res. 2022 Jan 1;480(1):79-81. doi: 10.1097/CORR.0000000000001975. Clin Orthop Relat Res. 2022. PMID: 34543252 Free PMC article. No abstract available.
Similar articles
-
Does Patient-specific Functional Pelvic Tilt Affect Joint Contact Pressure in Hip Dysplasia? A Finite-element Analysis Study.Clin Orthop Relat Res. 2021 Aug 1;479(8):1712-1724. doi: 10.1097/CORR.0000000000001737. Clin Orthop Relat Res. 2021. PMID: 33787527 Free PMC article.
-
Does Acetabular Coverage Vary Between the Supine and Standing Positions in Patients with Hip Dysplasia?Clin Orthop Relat Res. 2019 Nov;477(11):2455-2466. doi: 10.1097/CORR.0000000000000898. Clin Orthop Relat Res. 2019. PMID: 31389893 Free PMC article.
-
Factors Associated With Abnormal Joint Contact Pressure After Periacetabular Osteotomy: A Finite-Element Analysis.J Arthroplasty. 2022 Oct;37(10):2097-2105.e1. doi: 10.1016/j.arth.2022.04.045. Epub 2022 May 5. J Arthroplasty. 2022. PMID: 35526756
-
Periacetabular osteotomy in the treatment of severe acetabular dysplasia. Surgical technique.J Bone Joint Surg Am. 2006 Mar;88 Suppl 1 Pt 1:65-83. doi: 10.2106/JBJS.E.00887. J Bone Joint Surg Am. 2006. PMID: 16510801 Review.
-
Posterior Pelvic Tilt Allows for Increased Hip Motion, While Anterior Pelvic Tilt Decreases Joint Stress: A Systematic Review of Biomechanical and Motion Analyses.Arthroscopy. 2025 Feb 26:S0749-8063(25)00142-2. doi: 10.1016/j.arthro.2025.02.021. Online ahead of print. Arthroscopy. 2025. PMID: 40021069 Review.
Cited by
-
[Progress in diagnosis and hip arthroscopic treatment of borderline developmental dysplasia of hip with Cam-type femoroacetabular impingement].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2023 May 15;37(5):629-634. doi: 10.7507/1002-1892.202301058. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2023. PMID: 37190843 Free PMC article. Chinese.
-
Three-dimensional acetabular reorientation during periacetabular osteotomy: an intraoperative navigation method using an external fixator for periacetabular osteotomy.Arch Orthop Trauma Surg. 2024 Nov;144(11):4969-4977. doi: 10.1007/s00402-024-05590-1. Epub 2024 Sep 24. Arch Orthop Trauma Surg. 2024. PMID: 39313642
-
Providing a computationally derived, mechanically optimised target correction during preoperative planning can improve joint contact mechanics of hip dysplasia treated with periacetabular osteotomy.Hip Int. 2024 May;34(3):378-389. doi: 10.1177/11207000231212403. Epub 2023 Dec 10. Hip Int. 2024. PMID: 38073284 Free PMC article.
-
Finite element analyses, 3D-printed guides and navigation system optimizes fragment reorientation for periacetabular osteotomy.Int J Comput Assist Radiol Surg. 2025 Apr 26. doi: 10.1007/s11548-025-03376-3. Online ahead of print. Int J Comput Assist Radiol Surg. 2025. PMID: 40285833
-
Evaluation of the anterior acetabular coverage with a false profile radiograph considering appropriate range of positioning.Sci Rep. 2023 May 22;13(1):8288. doi: 10.1038/s41598-023-35514-9. Sci Rep. 2023. PMID: 37217756 Free PMC article.
References
-
- Bergmann G, Deuretzbacher G, Heller M, et al. Hip contact forces and gait patterns from routine activities. J Biomech. 2001;34:859-871. - PubMed
