

Toward Replacing Late Gadolinium Enhancement With Artificial Intelligence Virtual Native Enhancement for Gadolinium-Free Cardiovascular Magnetic Resonance Tissue Characterization in Hypertrophic Cardiomyopathy
- PMID: 34229451
- PMCID: PMC8378544
- DOI: 10.1161/CIRCULATIONAHA.121.054432
Toward Replacing Late Gadolinium Enhancement With Artificial Intelligence Virtual Native Enhancement for Gadolinium-Free Cardiovascular Magnetic Resonance Tissue Characterization in Hypertrophic Cardiomyopathy
Abstract
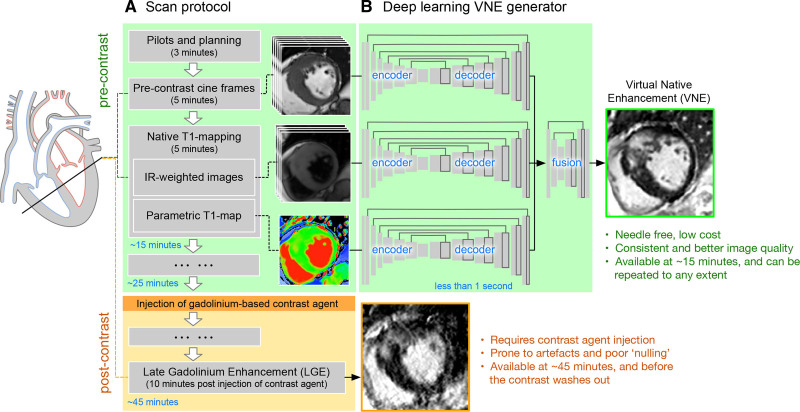
Background: Late gadolinium enhancement (LGE) cardiovascular magnetic resonance (CMR) imaging is the gold standard for noninvasive myocardial tissue characterization but requires intravenous contrast agent administration. It is highly desired to develop a contrast agent-free technology to replace LGE for faster and cheaper CMR scans.
Methods: A CMR virtual native enhancement (VNE) imaging technology was developed using artificial intelligence. The deep learning model for generating VNE uses multiple streams of convolutional neural networks to exploit and enhance the existing signals in native T1 maps (pixel-wise maps of tissue T1 relaxation times) and cine imaging of cardiac structure and function, presenting them as LGE-equivalent images. The VNE generator was trained using generative adversarial networks. This technology was first developed on CMR datasets from the multicenter Hypertrophic Cardiomyopathy Registry, using hypertrophic cardiomyopathy as an exemplar. The datasets were randomized into 2 independent groups for deep learning training and testing. The test data of VNE and LGE were scored and contoured by experienced human operators to assess image quality, visuospatial agreement, and myocardial lesion burden quantification. Image quality was compared using a nonparametric Wilcoxon test. Intra- and interobserver agreement was analyzed using intraclass correlation coefficients (ICC). Lesion quantification by VNE and LGE were compared using linear regression and ICC.
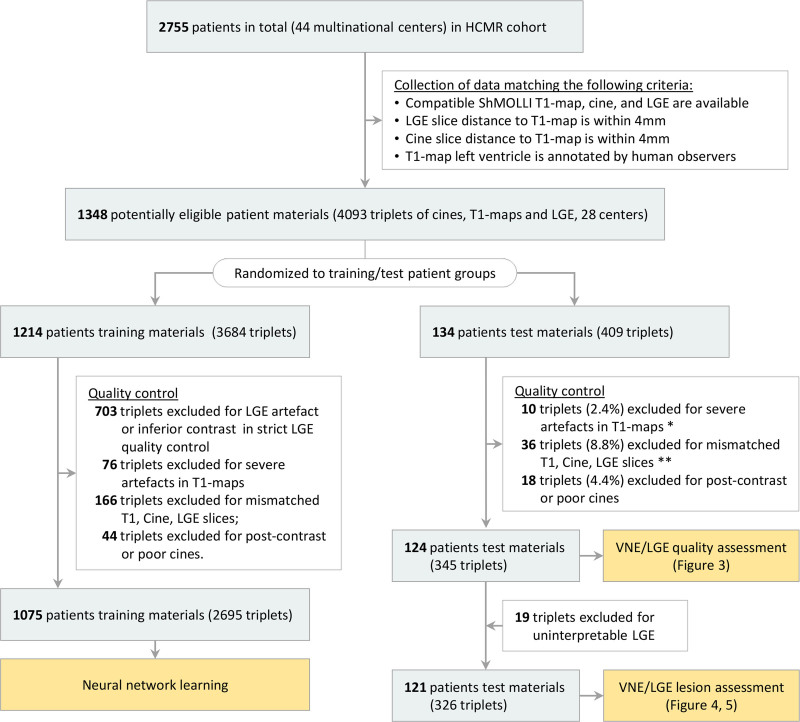
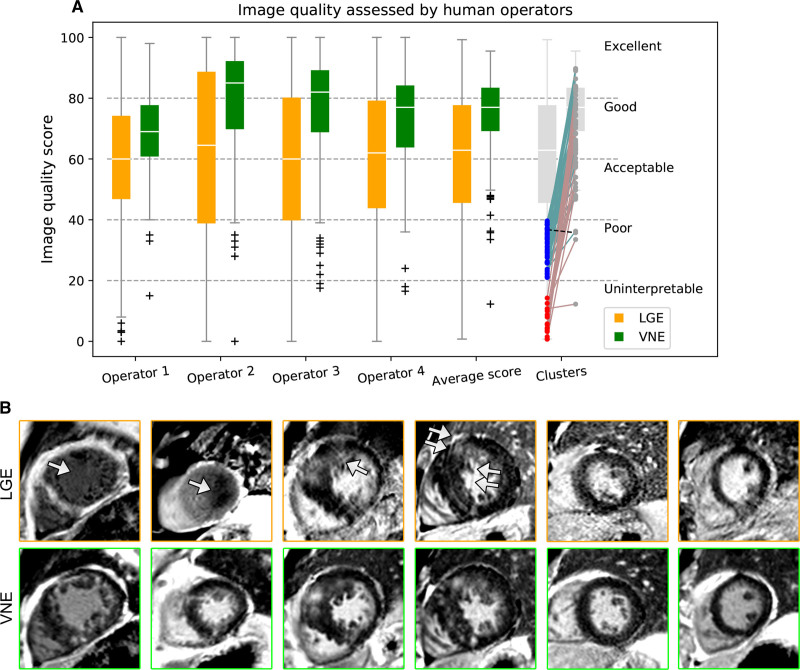
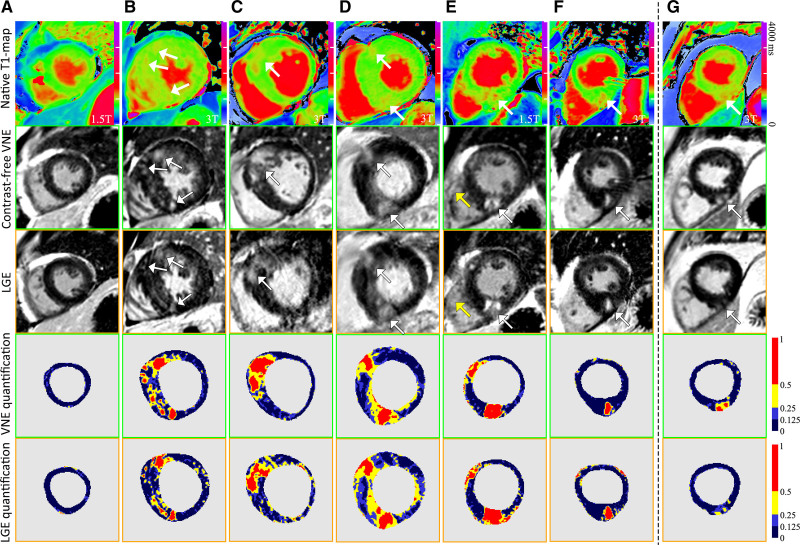
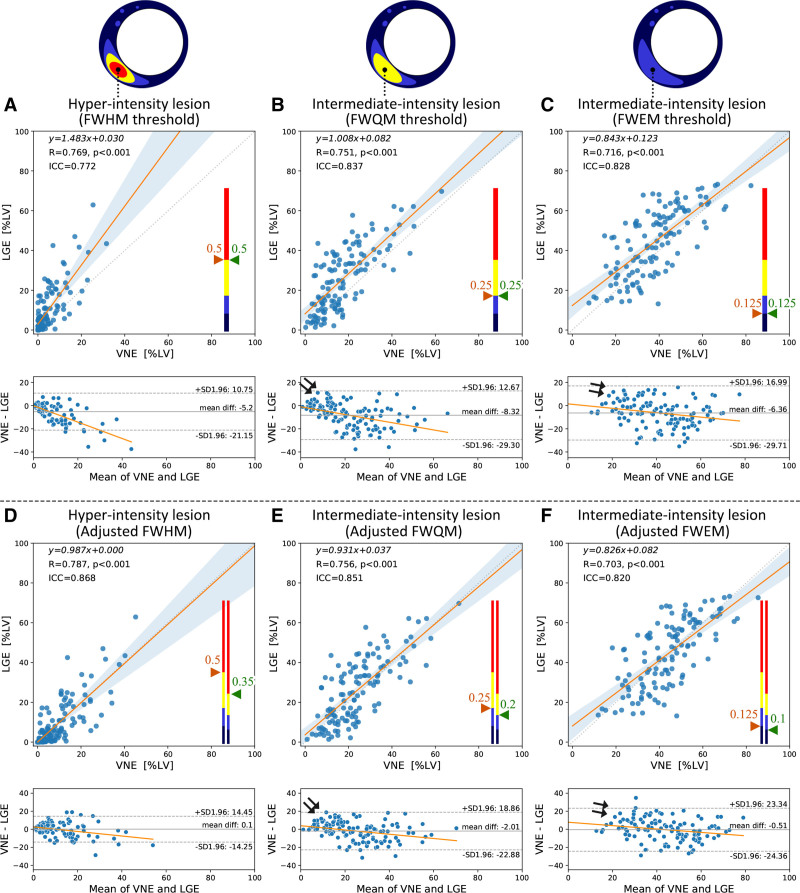
Results: A total of 1348 hypertrophic cardiomyopathy patients provided 4093 triplets of matched T1 maps, cines, and LGE datasets. After randomization and data quality control, 2695 datasets were used for VNE method development and 345 were used for independent testing. VNE had significantly better image quality than LGE, as assessed by 4 operators (n=345 datasets; P<0.001 [Wilcoxon test]). VNE revealed lesions characteristic of hypertrophic cardiomyopathy in high visuospatial agreement with LGE. In 121 patients (n=326 datasets), VNE correlated with LGE in detecting and quantifying both hyperintensity myocardial lesions (r=0.77-0.79; ICC=0.77-0.87; P<0.001) and intermediate-intensity lesions (r=0.70-0.76; ICC=0.82-0.85; P<0.001). The native CMR images (cine plus T1 map) required for VNE can be acquired within 15 minutes and producing a VNE image takes less than 1 second.
Conclusions: VNE is a new CMR technology that resembles conventional LGE but without the need for contrast administration. VNE achieved high agreement with LGE in the distribution and quantification of lesions, with significantly better image quality.
Keywords: artificial intelligence; cardiomyopathy, hypertrophic; contrast media; deep learning; gadolinium; magnetic resonance imaging.
Figures
Comment in
-
Automated Noncontrast Myocardial Tissue Characterization for Hypertrophic Cardiomyopathy: Holy Grail or False Prophet?Circulation. 2021 Aug 24;144(8):600-603. doi: 10.1161/CIRCULATIONAHA.121.055791. Epub 2021 Aug 23. Circulation. 2021. PMID: 34424773 No abstract available.
References
-
- Kim RJ, Wu E, Rafael A, Chen EL, Parker MA, Simonetti O, Klocke FJ, Bonow RO, Judd RM. The use of contrast-enhanced magnetic resonance imaging to identify reversible myocardial dysfunction. N Engl J Med. 2000;343:1445–1453. doi: 10.1056/NEJM200011163432003 - PubMed
-
- Bruder O, Wagner A, Lombardi M, Schwitter J, van Rossum A, Pilz G, Nothnagel D, Steen H, Petersen S, Nagel E, et al. European cardiovascular magnetic resonance (EuroCMR) registry – multi national results from 57 centers in 15 countries. J Cardiovasc MRI. 2013;15:9. doi: 10.1186/1532-429X-15-9 - PMC - PubMed
-
- Mahrholdt H, Wagner A, Judd RM, Sechtem U, Kim RJ. Delayed enhancement cardiovascular magnetic resonance assessment of non-ischaemic cardiomyopathies. Eur Heart J. 2005;26:1461–1474. doi: 10.1093/eurheartj/ehi258 - PubMed
-
- Becker MAJ, Cornel JH, van de Ven PM, van Rossum AC, Allaart CP, Germans T. The prognostic value of late gadolinium-enhanced cardiac magnetic resonance imaging in nonischemic dilated cardiomyopathy: a review and meta-analysis. JACC Cardiovasc Imag. 2018;11:1274–1284. doi: 10.1016/j.jcmg.2018.03.006 - PubMed
-
- Gerber BL, Rousseau MF, Ahn SA, le Polain de Waroux JB, Pouleur AC, Phlips T, Vancraeynest D, Pasquet A, Vanoverschelde JL. Prognostic value of myocardial viability by delayed-enhanced magnetic resonance in patients with coronary artery disease and low ejection fraction: impact of revascularization therapy. J Am Coll Cardiol. 2012;59:825–835. doi: 10.1016/j.jacc.2011.09.073 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
