

Pancreatic outflow tract reconstruction after pancreaticoduodenectomy: a meta-analysis of randomized controlled trials
- PMID: 34229720
- PMCID: PMC8262038
- DOI: 10.1186/s12957-021-02314-2
Pancreatic outflow tract reconstruction after pancreaticoduodenectomy: a meta-analysis of randomized controlled trials
Abstract
Background: To evaluate the outcomes of pancreaticogastrostomy and pancreaticojejunostomy after pancreatoduodenectomy with the help of a meta-analysis.
Methods: Randomized controlled trials comparing pancreaticogastrostomy and pancreaticojejunostomy were searched electronically using PubMed, The Cochrane Library, and EMBASE. Fixed and random-effects were used to measure pooled estimates. Research indicators included pancreatic fistula, delayed gastric emptying, postoperative hemorrhage, intraperitoneal fluid collection, wound infection, overall postoperative complications, reoperation, and mortality.
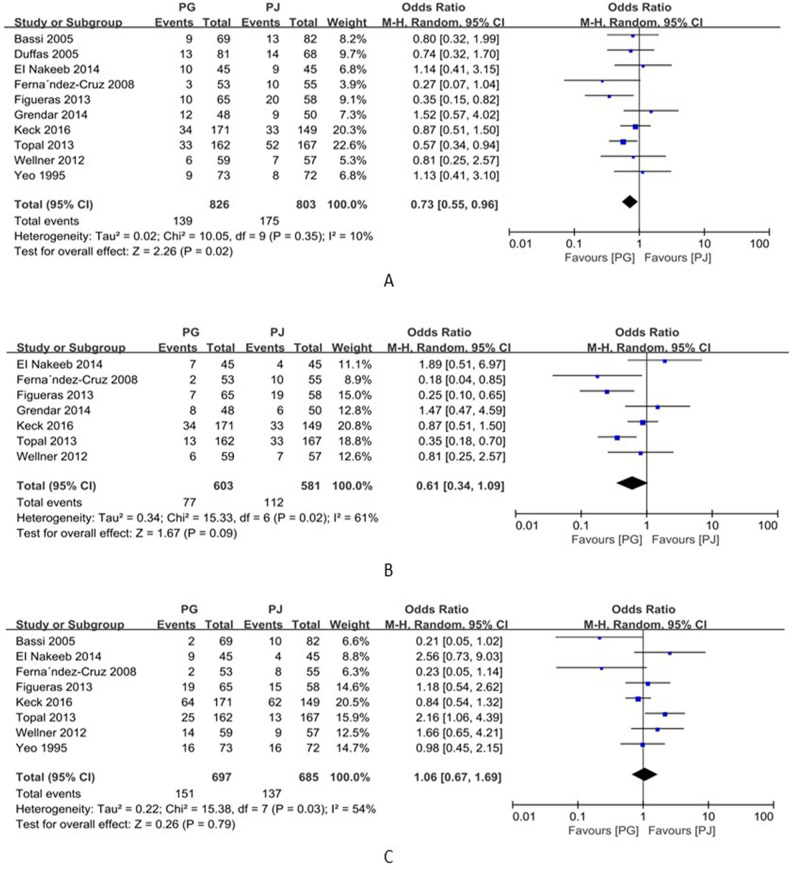
Results: Overall, 10 randomized controlled trials were included in this meta-analysis, with a total of 1629 patients. The overall incidences of pancreatic fistula and intra-abdominal collections were lower in the pancreaticogastrostomy group than in the pancreaticojejunostomy group (OR=0.73, 95% CI 0.55~0.96, p=0.02; OR=0.59, 95% CI 0.37~0.96, p=0.02, respectively). The incidence of B/C grade pancreatic fistula in the pancreaticogastrostomy group was lower than that in the pancreaticojejunostomy group, but no significant difference was observed (OR=0.61, 95%CI 0.34~1.09, p=0.09). Postoperative hemorrhage was more frequent in the pancreaticogastrostomy group than in the pancreaticojejunostomy group (OR=1.52; 95% CI 1.08~2.14, p=0.02). No significant differences in terms of delayed gastric emptying, wound infection, reoperation, overall postoperative complications, mortality, exocrine function, and hospital readmission were observed between groups.
Conclusion: This meta-analysis suggests that pancreaticogastrostomy reduces the incidence of postoperative pancreatic fistula and intraperitoneal fluid collection but increases the risk of postoperative hemorrhage compared with pancreaticojejunostomy.
Keywords: Delayed gastric emptying; Meta-analysis; Pancreatic fistula; Pancreaticoduodenectomy; Pancreaticogastrostomy; Pancreaticojejunostomy.
Conflict of interest statement
We confirm that the manuscript has been read and approved by all named authors and that there are no other persons who satisfied the criteria for authorship but are not listed. We further confirm that the order of authors listed in the manuscript has been approved by all of us. We also declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
We understand that the corresponding author is the sole contact for the editorial process. He is responsible for communicating with the other authors about progress, submissions of revisions, and final approval of proofs.
Figures





References
-
- Kimura W, Miyata H, Gotoh M, Hirai I, Kenjo A, Kitagawa Y, Shimada M, Baba H, Tomita N, Nakagoe T, Sugihara K, Mori M. A pancreaticoduodenectomy risk model derived from 8575 cases from a national single-race population (Japanese) using a web-based data entry system: the 30-day and in-hospital mortality rates for pancreaticoduodenectomy. Annals of surgery. 2014;259(4):773–780. doi: 10.1097/SLA.0000000000000263. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
