

Adaptive servo ventilation for sleep apnoea in heart failure: the FACE study 3-month data
- PMID: 34230094
- PMCID: PMC8762030
- DOI: 10.1136/thoraxjnl-2021-217205
Adaptive servo ventilation for sleep apnoea in heart failure: the FACE study 3-month data
Abstract
Rationale: Adaptive servo ventilation (ASV) is contraindicated in patients with systolic heart failure (HF) who have a left ventricular ejection fraction (LVEF) below 45% and predominant central sleep apnoea (CSA). However, the effects of ASV in other HF subgroups have not been clearly defined.
Objective: The European, multicentre, prospective, observational cohort trial, FACE, evaluated the effects of ASV therapy on morbidity and mortality in patients with HF with sleep-disordered breathing (SDB); 3-month outcomes in patient subgroups defined using latent class analysis (LCA) are presented.
Methods: Consecutive patients with HF with predominant CSA (±obstructive sleep apnoea) indicated for ASV were included from 2009 to 2018; the non-ASV group included patients who refused/were noncompliant with ASV. The primary endpoint was time to composite first event (all-cause death, lifesaving cardiovascular intervention or unplanned hospitalisation for worsening of chronic HF).
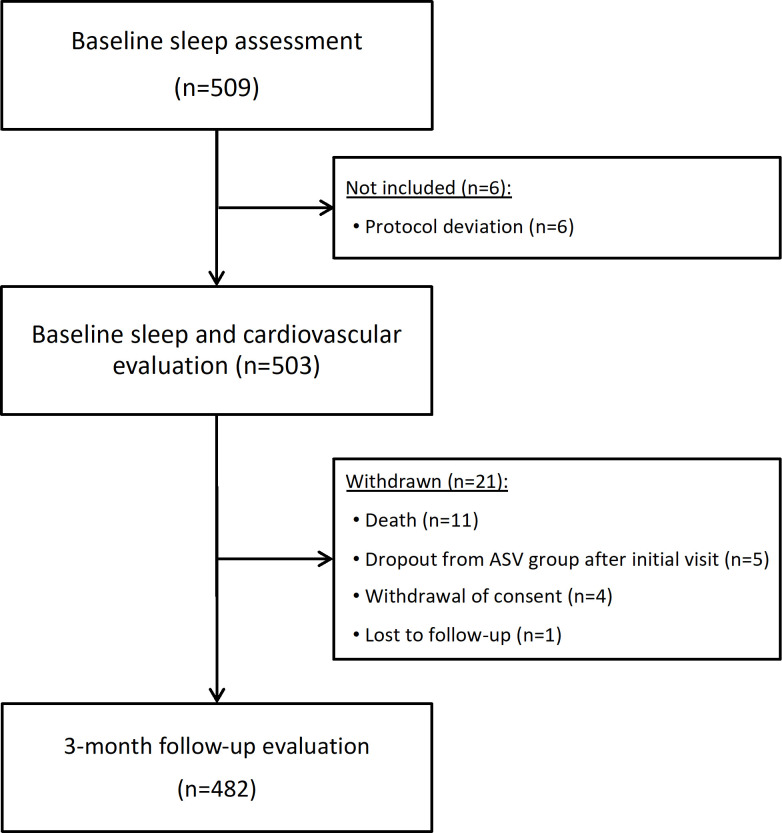
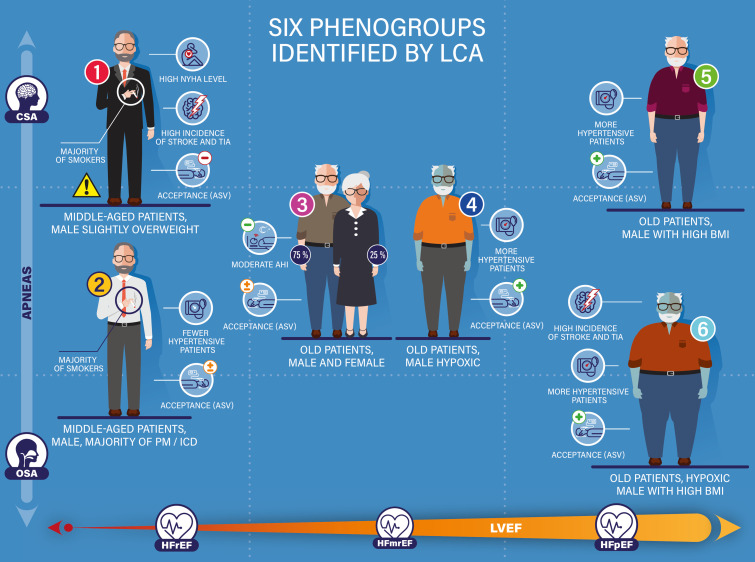
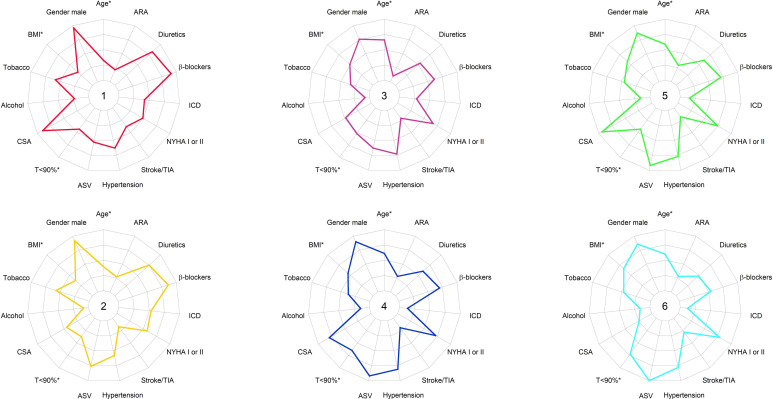
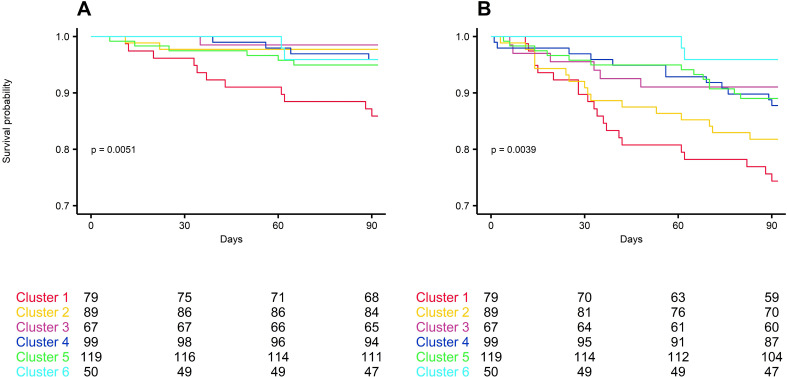
Measurements and main results: Baseline assessments were performed in 503 patients, and 482 underwent 3-month follow-up. LCA identified six discrete patient clusters characterised by variations in LVEF, SDB type, age, comorbidities and ASV acceptance. The 3- month rate of primary outcome events was significantly higher in cluster 1 patients (predominantly men, low LVEF, severe HF, CSA; 13.9% vs 1.5%-5% in other clusters, p<0.01).
Conclusion: For the first time, our data identified homogeneous patient clusters representing clinically relevant subgroups relating to SDB management in patients with HF with different ASV usage, each with a different prognosis. This may improve patient phenotyping in clinical practice and allow individualisation of therapy.
Keywords: sleep apnoea.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: JLP, TD, JMD, RT and MPO are FACE study investigators and steering committee members for ResMed. AP and FG are FACE study investigators for ResMed. RT has received unrestricted research grants from ResMed, Vitalaire, Philips and the AGPMC Foundation, consultant fees from ResMed, Inspire, Navigant and Jazz Pharmaceuticals, and travel grants from Agiradom. TD reports grants and fees from Pfizer, ResMed, GSK, Alnylam, Akcea Therapeutics, Ionis, Sanofi-Aventis, and Novartis. JAV reports grants and personal fees from ResMed, Bioproject and Jazz Pharmaceuticals, personal fees from Philips, Sanofi, Agfa-Gevaert and Springer, and grants from AirLiquide, Westfalen Medical, SomnoMed, Vivisol, Total Care, Medidis, Fisher & Paykel, Wave Medical, OSG, MediqTefa, NightBalance, Heinen & Löwenstein, AstraZeneca, Accuramed, Bekaert Deslee Academy and UCB Pharma, all outside the submitted work. MPO. has received unrestricted research grants from ResMed and Philips, consultant fees from ResMed, Somnomed and Jazz Pharmaceuticals, speaker fees from ResMed, Philips, LinaNova and Jazz Pharmaceuticals, and travelling grants from ISIS medical, Orkyn, SOS Oxygene and Vitalaire. SB has no conflicts of interest to declare. FL is an employee of ResMed.
Figures
Comment in
-
Central sleep apnoea in heart failure: one size does not fit all.Thorax. 2022 Feb;77(2):108-109. doi: 10.1136/thoraxjnl-2021-217694. Epub 2021 Jul 23. Thorax. 2022. PMID: 34301739 No abstract available.
References
-
- Ponikowski P, Voors AA, Anker SD, et al. . 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J 2016;37:2129–200. 10.1093/eurheartj/ehw128 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous