

Indocyanine green (ICG) fluorescent cholangiography during laparoscopic cholecystectomy using RUBINA™ technology: preliminary experience in two pediatric surgery centers
- PMID: 34231069
- PMCID: PMC8523512
- DOI: 10.1007/s00464-021-08596-7
Indocyanine green (ICG) fluorescent cholangiography during laparoscopic cholecystectomy using RUBINA™ technology: preliminary experience in two pediatric surgery centers
Abstract
Background: Recently, we reported the feasibility of indocyanine green (ICG) near-infrared fluorescence (NIRF) imaging to identify extrahepatic biliary anatomy during laparoscopic cholecystectomy (LC) in pediatric patients. This paper aimed to describe the use of a new technology, RUBINA™, to perform intra-operative ICG fluorescent cholangiography (FC) in pediatric LC.
Methods: During the last year, ICG-FC was performed during LC using the new technology RUBINA™ in two pediatric surgery units. The ICG dosage was 0.35 mg/Kg and the median timing of administration was 15.6 h prior to surgery. Patient baseline, intra-operative details, rate of biliary anatomy identification, utilization ease, and surgical outcomes were assessed.
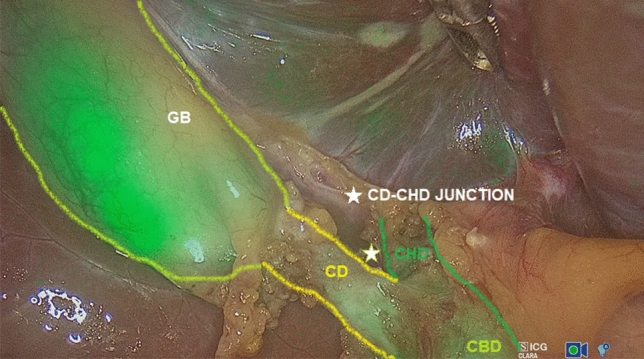
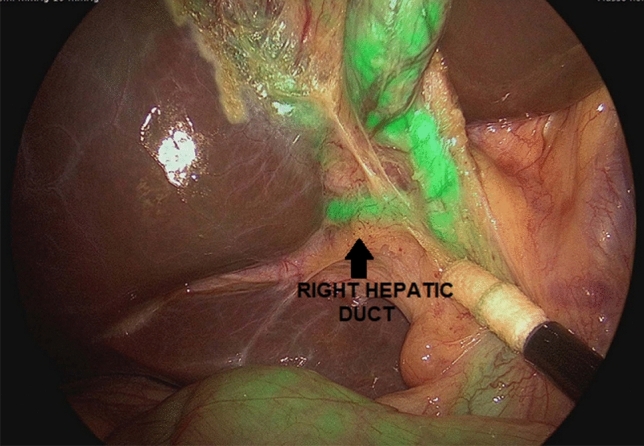
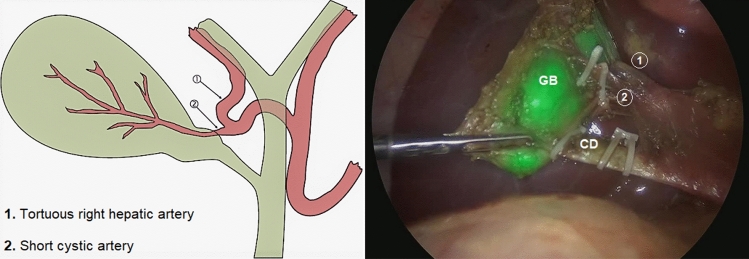
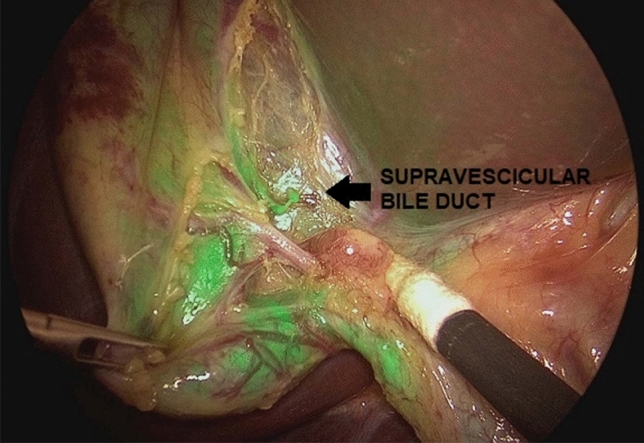
Results: Thirteen patients (11 girls), with median age at surgery of 12.9 years, underwent LC using the new RUBINA™ technology. Six patients (46.1%) had associated comorbidities and five (38.5%) were practicing drug therapy. Pre-operative workup included ultrasound (n = 13) and cholangio-MRI (n = 5), excluding biliary and/or vascular anatomical anomalies. One patient needed conversion to open surgery and was excluded from the study. The median operative time was 96.9 min (range 55-180). Technical failure of intra-operative ICG-NIRF visualization occurred in 2/12 patients (16.7%). In the other cases, ICG-NIRF allowed to identify biliary/vascular anatomic anomalies in 4/12 (33.3%), including Moynihan's hump of the right hepatic artery (n = 1), supravescicular bile duct (n = 1), and short cystic duct (n = 2). No allergic or adverse reactions to ICG, post-operative complications, or reoperations were reported.
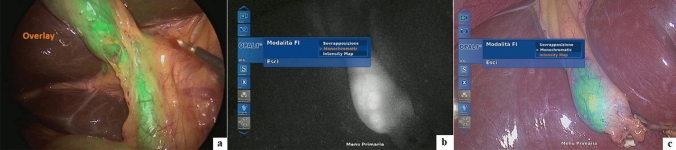
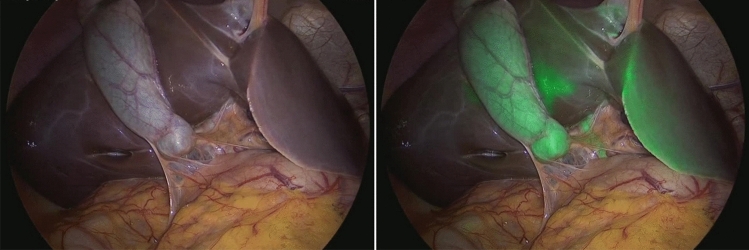
Conclusion: Our preliminary experience suggested that the new RUBINA™ technology was very effective to perform ICG-FC during LC in pediatric patients. The advantages of this technology include the possibility to overlay the ICG-NIRF data onto the standard white light image and provide surgeons a constant fluorescence imaging of the target anatomy to assess position of critical biliary structures or presence of anatomical anomalies and safely perform the operation.
Keywords: Children; Cholangiography; Cholecystectomy; Fluorescence; Indocyanine green; Technology.
© 2021. The Author(s).
Conflict of interest statement
Drs Ciro Esposito, Daniele Alberti, Alessandro Settimi, Silvia Pecorelli, Giovanni Boroni, Beatrice Montanaro, and Maria Escolino declare that they have no conflict of interest or financial ties to disclose.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
