

Association Between Disease-Modifying Therapies Prescribed to Persons with Multiple Sclerosis and Cancer: a WHO Pharmacovigilance Database Analysis
- PMID: 34231126
- PMCID: PMC8608969
- DOI: 10.1007/s13311-021-01073-y
Association Between Disease-Modifying Therapies Prescribed to Persons with Multiple Sclerosis and Cancer: a WHO Pharmacovigilance Database Analysis
Abstract
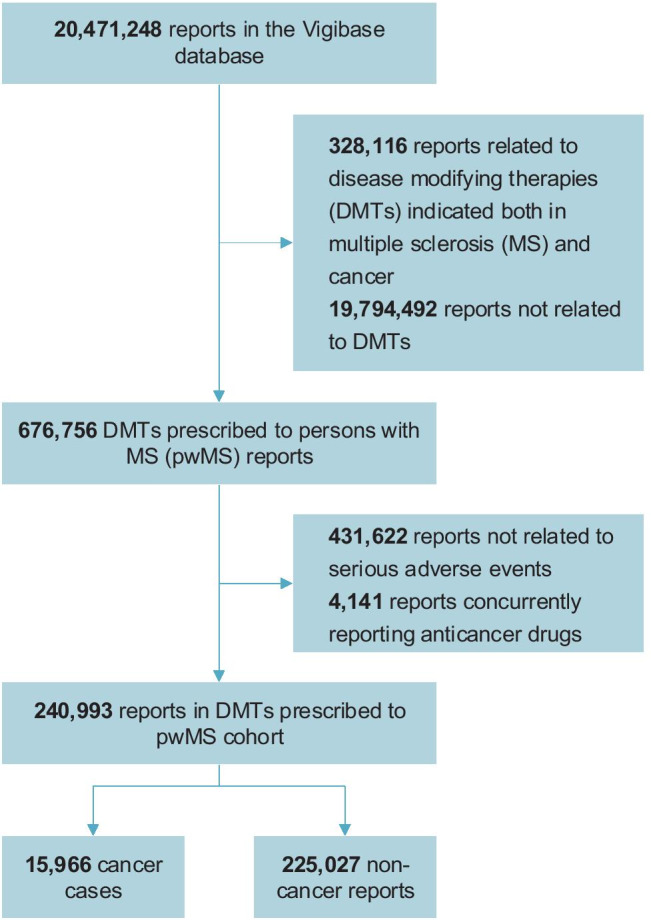
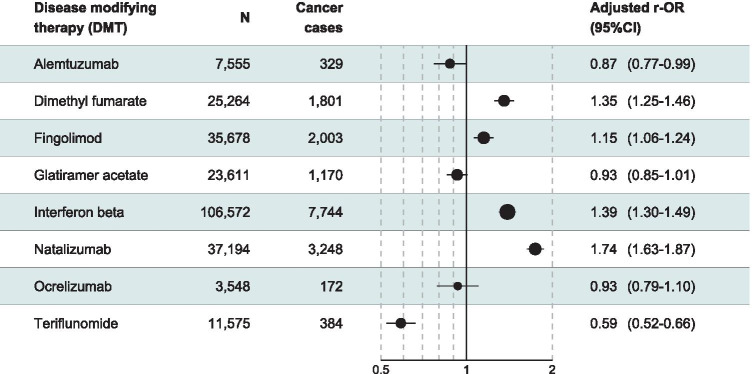
The risk of cancer associated with persons with multiple sclerosis (pwMS) prescribed with disease modifying therapies (DMTs) is not well established. This observational, cross-sectional, pharmacovigilance cohort study examined individual case safety reports from the World Health Organization database: VigiBase®. All consecutive reports of DMTs prescribed to pwMS (alemtuzumab, dimethyl fumarate, fingolimod, glatiramer acetate, interferon-β, natalizumab, ocrelizumab, and teriflunomide), and their serious adverse event cases were eligible, excluding those reporting immunosuppressant DMTs used as anticancer therapies. The primary outcome was the multivariate odds ratio of cancer reporting (r-OR) for DMTs prescribed to pwMS after imputation of missing data. There were 5966 cancer cases from 240,993 reports of DMTs prescribed to pwMS. After adjustments on age, sex, and geographical region, natalizumab (r-OR 1.74, 95% CI 1.63-1.87), interferon-β (r-OR 1.39, 95% CI 1.30-1.49), dimethyl fumarate (r-OR 1.35, 95% CI 1.25-1.46), and fingolimod (r-OR 1.15, 95% CI 1.06-1.24) were significantly associated with a greater cancer reporting, whereas alemtuzumab, glatiramer acetate, ocrelizumab, and teriflunomide were not, in the disproportionality analysis. As exploratory analyses, upper aerodigestive tract, breast, urinary including the male genitourinary tract, and nervous system cancers were associated with natalizumab, interferon-β, and dimethyl fumarate. Fingolimod was only associated with skin cancer types. Cancer cases reporting these four DMTs prescribed to pwMS were younger in age than for non-pwMS drugs in the VigiBase® (p < 0.0001). A close and regular cancer screening in pwMS treated with natalizumab, interferon-β, dimethyl fumarate, and fingolimod may be warranted, even for persons at a younger age. Trial Registration NCT04237337.
© 2021. The American Society for Experimental NeuroTherapeutics, Inc.
Conflict of interest statement
Charles Dolladille declares no competing interests.
Basile Chrétien declares no competing interests.
Laure Peyro-Saint-Paul declares no competing interests.
Joachim Alexandre declares no competing interests.
Olivier Dejardin declares no competing interests.
Sophie Fedrizzi declares no competing interests.
Gilles Defer has received personal compensation for the scientific advisory board for Biogen, Novartis, Genzyme, Merck Serono, Roche, and Teva. He has received speaker honoraria and travel grants from Merck Serono, Biogen, Novartis, Roche, Genzyme, and Teva. His institution has received research support in his department from Merck Serono, Biogen, Novartis, and Genzyme.
Figures
References
-
- Montalban X, Gold R, Thompson AJ, Otero-Romero S, Amato MP, Chandraratna D, et al. ECTRIMS/EAN Guideline on the pharmacological treatment of people with multiple sclerosis. Mult Scler J. :25. - PubMed
-
- Melamed E, Lee MW. Multiple Sclerosis and Cancer: The Ying-Yang Effect of Disease Modifying Therapies. Front Immunol [Internet]. 2020 Jan 10 [cited 2020 Apr 17];10. Available from: https://www.frontiersin.org/article/10.3389/fimmu.2019.02954/full - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
