

Adverse Local Tissue Reactions are Common in Asymptomatic Individuals After Hip Resurfacing Arthroplasty: Interim Report from a Prospective Longitudinal Study
- PMID: 34232144
- PMCID: PMC8726542
- DOI: 10.1097/CORR.0000000000001882
Adverse Local Tissue Reactions are Common in Asymptomatic Individuals After Hip Resurfacing Arthroplasty: Interim Report from a Prospective Longitudinal Study
Abstract
Background: The evaluation of the natural history prevalence of adverse local tissue reactions (ALTRs) using MRI has focused only on metal-on-metal (MoM) bearing surfaces without comparison to nonMoM bearing surfaces.
Questions/purposes: To determine (1) the longitudinal changes and differences in blood metal ion levels in patients with hip resurfacing arthroplasty (HRA), ceramic-on-ceramic (CoC) THA, and metal-on-polyethylene (MoP) THA compared with those undergoing ceramic-on-polyethylene (CoP) THA; (2) how the longitudinal change of synovial reaction classification in patients with HRA, CoC THA, and MoP THA compares with those undergoing CoP THA, and whether there is an association between the presence of an ALTR or metallosis on MRI with corresponding patient-reported outcomes, or the presence of capsular dehiscence; and (3) differences in blood metal ion levels between patients undergoing HRA with an ALTR or metallosis on MRI and those with HRA without these conditions.
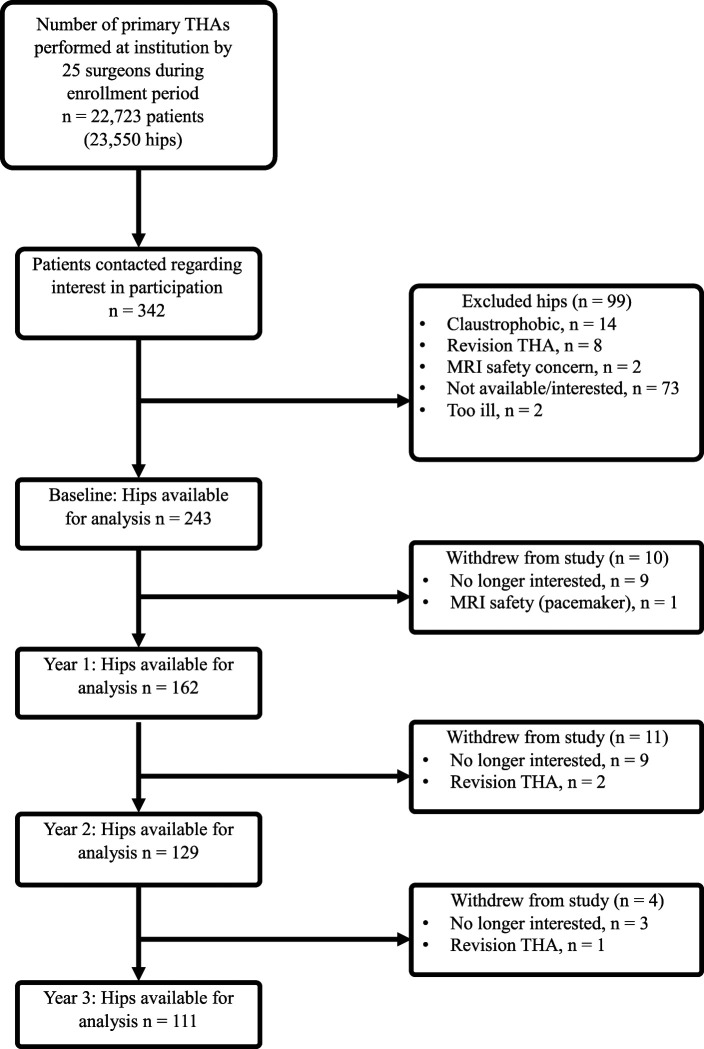
Methods: Between March 2014 and February 2019, 22,723 patients underwent primary HRA and THA at one center. Patients received an HRA based on their desired athletic level after surgery and the presence of normal acetabular and proximal femoral bone morphology without osteopenia or osteoporosis. Two percent (342 of 22,723) of patients were contacted to participate, and 71% (243 of 342 hips in 206 patients) were enrolled for analysis at baseline. The patients underwent arthroplasty for degenerative joint disease, and 25 patients withdrew over the course of the study. We included patients who were more than 1 year postarthroplasty. All participants had an MRI examination and blood serum ion testing and completed a Hip Disability and Osteoarthritis Outcome Score survey annually for four years (baseline, year 1, year 2, year 3). Morphologic and susceptibility-reduced MR images were evaluated by a single radiologist not involved in the care of patients for the presence and classification of synovitis (Gwet AC1: 0.65 to 0.97), synovial thickness, and volume (coefficient of repeatability: 1.8 cm3). Linear mixed-effects models were used to compare the mean synovial thickness, synovial volume, and Hip Disability and Osteoarthritis Outcome Score subscales between bearing surfaces at each timepoint and within each bearing surface over time. Marginal Cox proportional hazards models were used to compare the time to and the risk of developing ALTR only, metallosis only, and ALTR or metallosis between bearing surfaces. All models were adjusted for age, sex, BMI, and length of implantation based on known confounders for hip arthroplasty. Adjustment for multiple comparisons was performed using the Dunnett-Hsu method.
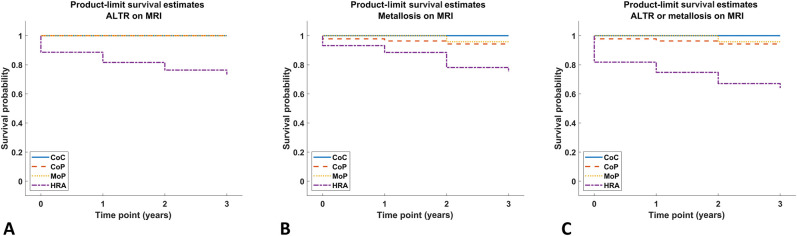
Results: Patients with unilateral HRA had higher cobalt and chromium serum ion levels (baseline: 1.8 ± 0.8 ppb, year 1: 2.0 ± 1.5 ppb, year 2: 2.1 ± 1.2 ppb, year 3: 1.6 ± 0.7 ppb) than those with unilateral CoP bearings (baseline: 0.0 ± 0.1 ppb, year 1: 0.1 ± 0.3 ppb, year 2: 0.0 ± 0.2 ppb, year 3: 0.0 ± 0.0 ppb) at all timepoints (p < 0.001 for each time point). More patients who received an HRA developed ALTR or metallosis on MRI than did patients with CoP bearings (hazard ratio 4.8 [95% confidence interval 1.2 to 18.4]; p = 0.02). There was no association between the longitudinal change of synovial reaction to ALTR or metallosis on MRI with patient-reported outcomes. In addition, there was no association between the presence of dehiscence at baseline and the subsequent development of ALTR or metallosis, as seen on MRI. There were elevated cobalt (4.7 ± 3.5 ppb) and chromium (4.7 ± 2.6 ppb) serum levels in patients with unilateral HRA who had an ALTR or metallosis present on MRI at year 1 compared with patients without an ALTR or metallosis on MRI (cobalt: 1.8 ± 1.0 ppb, mean difference 4.7 ppb [95% CI 3.3 to 6.0]; p < 0.001; chromium: 2.3 ± 0.5 ppb, mean difference 3.6 ppb [95% CI 2.2 to 5.0]; p < 0.001) as well as for chromium at year 3 (3.9 ± 2.4 ppb versus 2.2 ± 1.1 ppb, mean difference 1.3 ppb [95% CI 0.3 to 2.4]; p = 0.01).
Conclusion: We found a higher proportion of ALTR or metallosis on MRI in patients with HRA compared with patients with CoP, even when patient self-assessed symptomatology of those with an ALTR or metallosis on MRI was not different than the absence of these features. MRI detected ALTRs in high-function patients, emphasizing that an annual clinical assessment dependent on survey or blood ion testing alone may not detect soft tissue complications. The results of this study are in line with prior consensus recommendations of using MRI as part of a routine follow-up protocol for this patient population.
Level of evidence: Level III, therapeutic study.
Copyright © 2021 by the Association of Bone and Joint Surgeons.
Conflict of interest statement
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research® editors and board members are on file with the publication and can be viewed on request.
Figures
Comment in
-
CORR Insights®: Adverse Local Tissue Reactions are Common in Asymptomatic Individuals After Hip Resurfacing Arthroplasty: Interim Report from a Prospective Longitudinal Study.Clin Orthop Relat Res. 2021 Dec 1;479(12):2651-2652. doi: 10.1097/CORR.0000000000001926. Clin Orthop Relat Res. 2021. PMID: 34351317 Free PMC article. No abstract available.
-
Letter to the Editor: Adverse Local Tissue Reactions are Common in Asymptomatic Individuals After Hip Resurfacing Arthroplasty: Interim Report from a Prospective Longitudinal Study.Clin Orthop Relat Res. 2022 Jul 1;480(7):1425-1426. doi: 10.1097/CORR.0000000000002214. Epub 2022 May 3. Clin Orthop Relat Res. 2022. PMID: 35503306 Free PMC article. No abstract available.
-
Reply to the Letter to the Editor: Adverse Local Tissue Reactions are Common in Asymptomatic Individuals After Hip Resurfacing Arthroplasty: Interim Report from a Prospective Longitudinal Study.Clin Orthop Relat Res. 2022 Jul 1;480(7):1427-1429. doi: 10.1097/CORR.0000000000002229. Epub 2022 May 3. Clin Orthop Relat Res. 2022. PMID: 35503436 Free PMC article. No abstract available.
References
-
- Barlow BT, Ortiz PA, Fields KG, Burge AJ, Potter HG, Westrich GH. Magnetic resonance imaging predicts adverse local tissue reaction histologic severity in modular neck total hip arthroplasty. J Arthroplasty. 2016;31:2325-2331. - PubMed
-
- Barrack RL, Sawhney J, Hsu J, Cofield RH. Cost analysis of revision total hip arthroplasty. A 5-year followup study. Clin Orthop Relat Res. 1999;369:175-178. - PubMed
-
- Bosker BH, Ettema HB, Boomsma MF, Kollen BJ, Maas M, Verheyen CCPM. High incidence of pseudotumour formation after large-diameter metal-on-metal total hip replacement: a prospective cohort study. J Bone Joint Surg Br. 2012;94:755-761. - PubMed
-
- Briant-Evans TW, Lyle N, Barbur S, et al. A longitudinal study of MARS MRI scanning of soft-tissue lesions around metal-on-metal total hip arthroplasties and disease progression. Bone Joint J. 2015;97-B:1328-1337. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
