

Non-invasive ventilatory support and high-flow nasal oxygen as first-line treatment of acute hypoxemic respiratory failure and ARDS
- PMID: 34232336
- PMCID: PMC8261815
- DOI: 10.1007/s00134-021-06459-2
Non-invasive ventilatory support and high-flow nasal oxygen as first-line treatment of acute hypoxemic respiratory failure and ARDS
Abstract
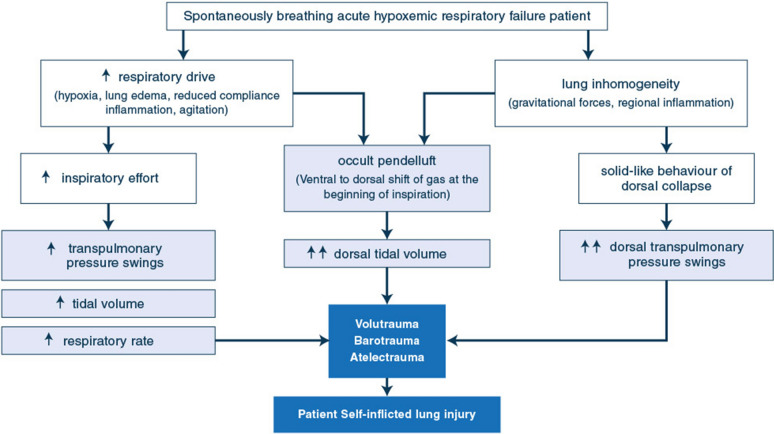
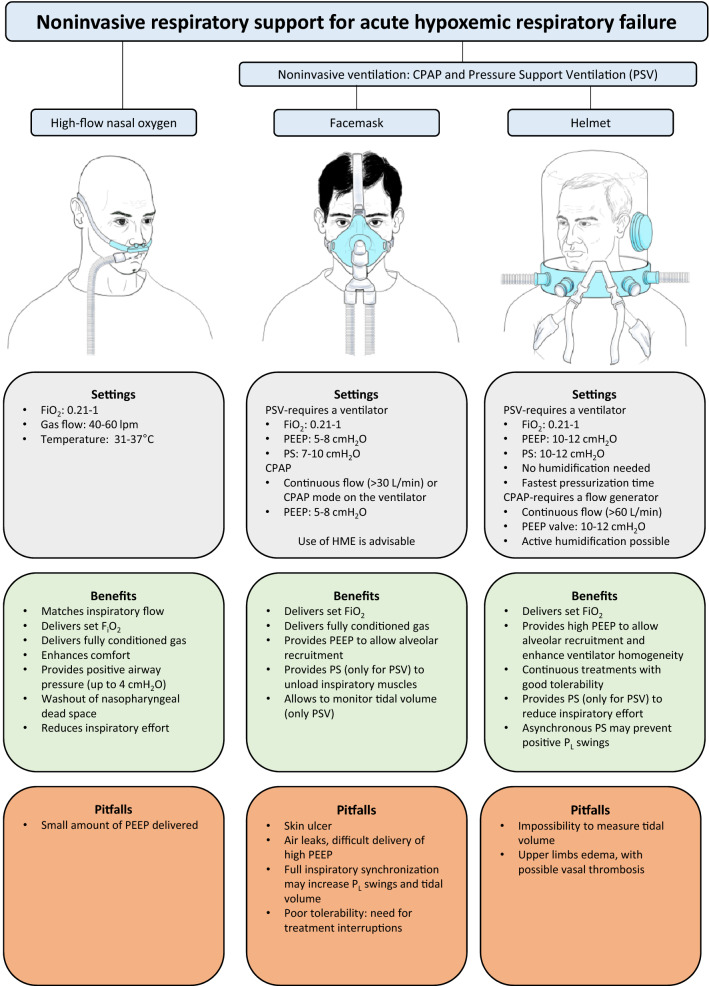
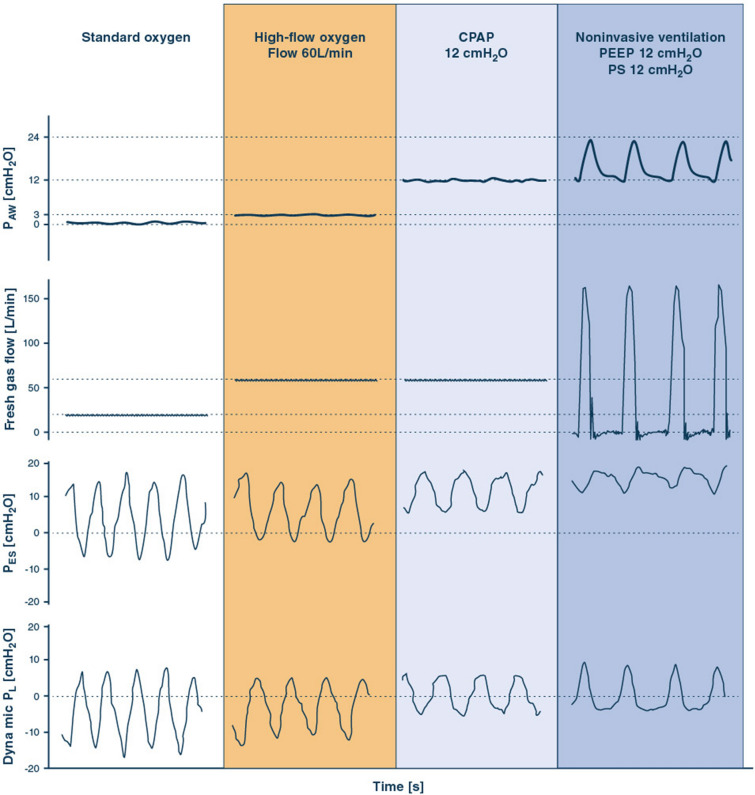
The role of non-invasive respiratory support (high-flow nasal oxygen and noninvasive ventilation) in the management of acute hypoxemic respiratory failure and acute respiratory distress syndrome is debated. The oxygenation improvement coupled with lung and diaphragm protection produced by non-invasive support may help to avoid endotracheal intubation, which prevents the complications of sedation and invasive mechanical ventilation. However, spontaneous breathing in patients with lung injury carries the risk that vigorous inspiratory effort, combined or not with mechanical increases in inspiratory airway pressure, produces high transpulmonary pressure swings and local lung overstretch. This ultimately results in additional lung damage (patient self-inflicted lung injury), so that patients intubated after a trial of noninvasive support are burdened by increased mortality. Reducing inspiratory effort by high-flow nasal oxygen or delivery of sustained positive end-expiratory pressure through the helmet interface may reduce these risks. In this physiology-to-bedside review, we provide an updated overview about the role of noninvasive respiratory support strategies as early treatment of hypoxemic respiratory failure in the intensive care unit. Noninvasive strategies appear safe and effective in mild-to-moderate hypoxemia (PaO2/FiO2 > 150 mmHg), while they can yield delayed intubation with increased mortality in a significant proportion of moderate-to-severe (PaO2/FiO2 ≤ 150 mmHg) cases. High-flow nasal oxygen and helmet noninvasive ventilation represent the most promising techniques for first-line treatment of severe patients. However, no conclusive evidence allows to recommend a single approach over the others in case of moderate-to-severe hypoxemia. During any treatment, strict physiological monitoring remains of paramount importance to promptly detect the need for endotracheal intubation and not delay protective ventilation.
Keywords: Acute hypoxemic respiratory failure (AHRF); Acute respiratory distress syndrome (ARDS); Continuous positive airway pressure (CPAP); High-flow nasal oxygen (H-FNO); Inspiratory effort; Noninvasive ventilation (NIV); Patient self-inflicted lung injury (P-SILI); Pressure support ventilation (PSV); Transpulmonary pressure.
© 2021. Springer-Verlag GmbH Germany, part of Springer Nature.
Conflict of interest statement
DLG has received payments for travel expenses by Maquet, Getinge and Air Liquide. MA has received personal fees by Maquet, and a research grant by Toray. TM received personal fees from Drager, Fisher and Paykel, BBraun and Mindray, outside of the submitted work. AWT has received personal fees (payments for lectures and travel expense coverage to attend scientific meetings) from Fisher & Paykel Healthcare, Maquet-Getinge, GE Healthcare, and Covidien. OR discloses a research grant from Hamilton Medical, he has received speaker fees from Hamilton Medical, Ambu and Aerogen Ltd, non-financial research support from Timpel and Masimo Corporation. JM reports personal fees from Faron, personal fees from Medtronic, personal fees from Janssen, and investigator-initiated grant from Covidien/Medtronic and CIHR, all outside the submitted work (last 36 months). DLG and MA disclose a research grant by General Electric Healthcare.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
