

Identifying the deceiver: the non-neoplastic mimickers of genital system neoplasms
- PMID: 34232414
- PMCID: PMC8263845
- DOI: 10.1186/s13244-021-01046-x
Identifying the deceiver: the non-neoplastic mimickers of genital system neoplasms
Abstract
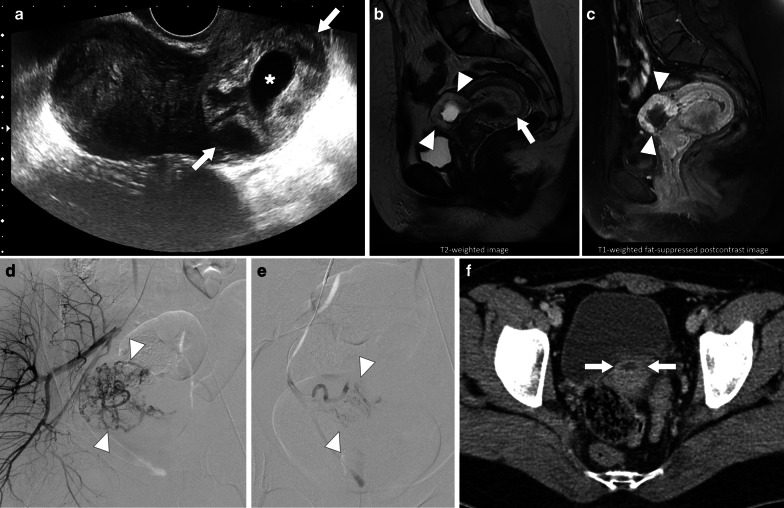
Tumors of the genital system are common and imaging is of crucial importance for their detection and diagnosis. Several non-neoplastic diseases may mimic these tumors and differential diagnosis may be difficult in certain cases. Misdiagnosing non-neoplastic diseases as tumor may prompt unnecessary medical treatment or surgical interventions. In this article, we aimed to present the imaging characteristics of non-neoplastic diseases of the male and female genital systems that may mimic neoplastic processes. Increasing awareness of the imaging specialists to these entities may have a severe positive impact on the management of these patients.
Keywords: Genital system; Infection; Inflammation; Mimicker; Neoplasm.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

































Similar articles
-
Imaging findings of infectious and inflammatory diseases of the urinary system mimicking neoplastic diseases.Abdom Radiol (NY). 2020 Apr;45(4):1110-1121. doi: 10.1007/s00261-019-02222-w. Abdom Radiol (NY). 2020. PMID: 31570959 Review.
-
Neoplastic Elbow Diseases and Mimickers.Semin Musculoskelet Radiol. 2021 Aug;25(4):600-616. doi: 10.1055/s-0041-1735608. Epub 2021 Oct 27. Semin Musculoskelet Radiol. 2021. PMID: 34706390 Review.
-
Pseudoneoplastic lesions of the female genital tract.Arch Pathol Lab Med. 2010 Mar;134(3):393-403. doi: 10.5858/134.3.393. Arch Pathol Lab Med. 2010. PMID: 20196667 Review.
-
Non-neoplastic cystic and cystic-like lesions of the pancreas: may mimic pancreatic cystic neoplasms.ANZ J Surg. 2006 May;76(5):325-31. doi: 10.1111/j.1445-2197.2006.03718.x. ANZ J Surg. 2006. PMID: 16768691
-
Endometriosis MR mimickers: T2-hypointense lesions.Insights Imaging. 2024 Jan 25;15(1):20. doi: 10.1186/s13244-023-01588-2. Insights Imaging. 2024. PMID: 38267633 Free PMC article. Review.
References
Publication types
LinkOut - more resources
Full Text Sources
