

Assessment of squamous cell carcinoma of the floor of the mouth with magnetic resonance imaging
- PMID: 34232443
- PMCID: PMC8639569
- DOI: 10.1007/s11604-021-01161-1
Assessment of squamous cell carcinoma of the floor of the mouth with magnetic resonance imaging
Abstract
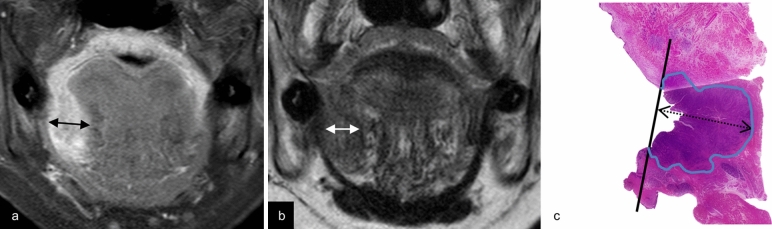
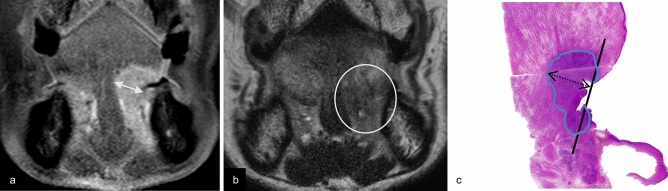
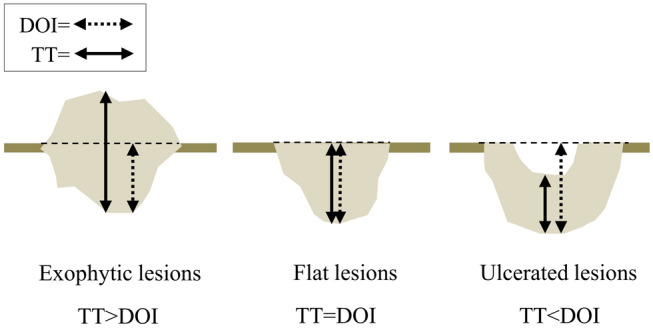
Purpose: We aimed to use magnetic resonance imaging (MRI) to determine the relationship between the pathological depth of invasion (DOI), undetectability, and tumor thickness of squamous cell carcinoma of the floor of the mouth.
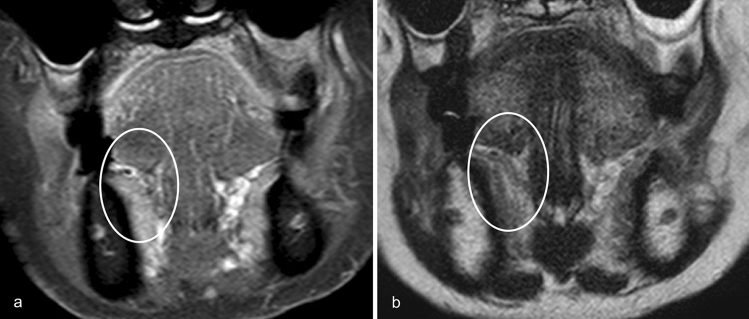
Materials and methods: We retrospectively evaluated the relationship between pathological DOI and MRI detectability, as well as the relationship between pathological DOI and tumor thickness on coronal fat-suppressed contrast-enhanced T1-weighted imaging or coronal T2-weighted imaging.
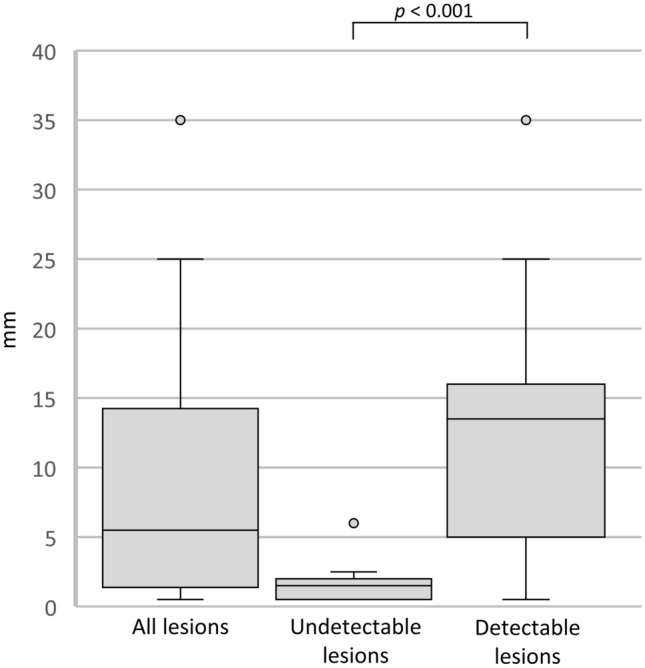
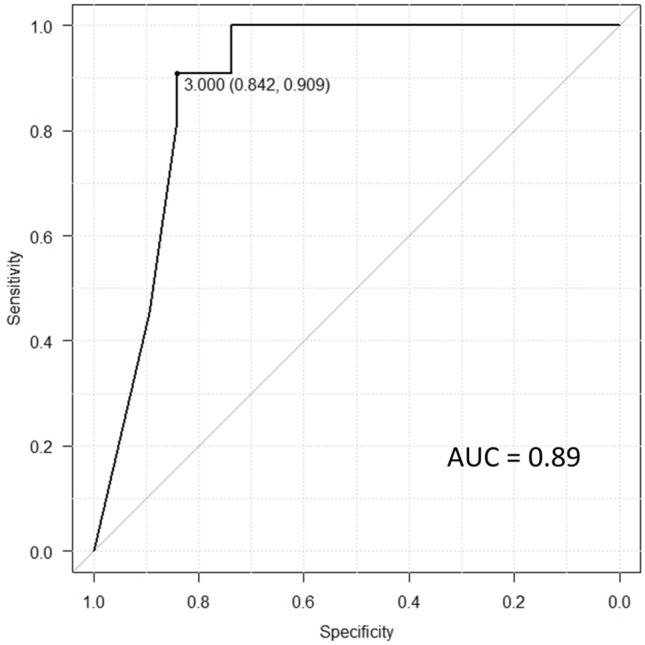
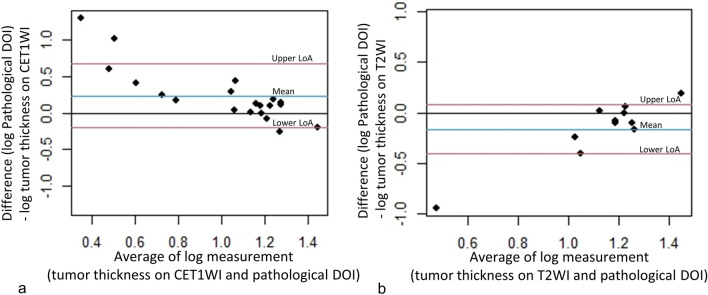
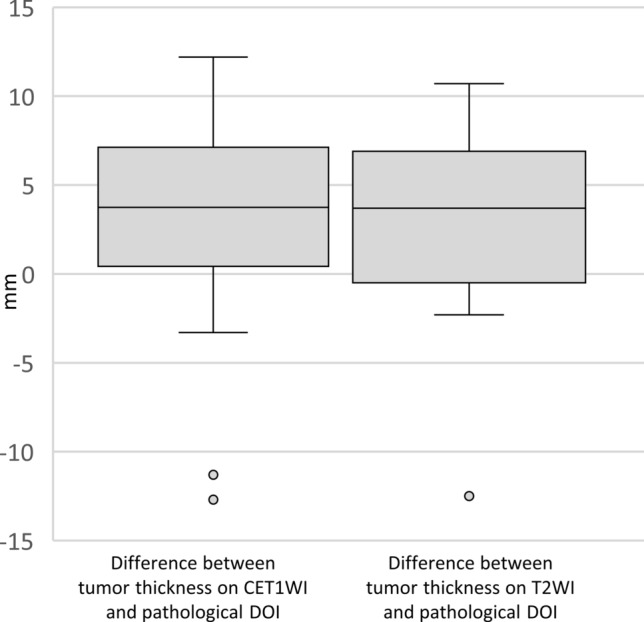
Results: We analyzed 30 patients with squamous cell carcinoma of the floor of the mouth; MRI revealed that the pathological DOI of the 11 undetectable lesions (median 2 mm) was smaller than that of the 19 detectable lesions (median 14 mm) (p < 0.001), and the cut-off value was 3 mm (sensitivity, 0.84; specificity, 0.91; area under the curve, 0.89). Tumor thickness on coronal fat-suppressed contrast-enhanced T1-weighted imaging was assessed in all 19 detectable lesions; however, tumor thickness on coronal T2-weighted imaging could not be assessed in eight cases. Tumor thickness on coronal fat-suppressed contrast-enhanced T1-weighted imaging was found to be significantly associated with the pathological DOI.
Conclusions: Undetectability on MRI indicates superficial lesions with a pathological DOI value that is less than 3 mm. In detectable lesions, tumor thickness on coronal fat-suppressed contrast-enhanced T1-weighted imaging is associated with pathological DOI.
Keywords: Carcinoma; Magnetic resonance imaging; Mouth floor; Neoplasm invasiveness; Squamous cell.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
Similar articles
-
Assessment of tumor depth in oral tongue squamous cell carcinoma with multiparametric MRI: correlation with pathology.Eur Radiol. 2022 Jan;32(1):254-261. doi: 10.1007/s00330-021-08148-6. Epub 2021 Jul 13. Eur Radiol. 2022. PMID: 34255162 Free PMC article.
-
Correlation between the magnetic resonance imaging features of squamous cell carcinoma of the buccal mucosa and pathologic depth of invasion.Oral Surg Oral Med Oral Pathol Oral Radiol. 2021 May;131(5):582-590. doi: 10.1016/j.oooo.2020.12.023. Epub 2021 Jan 8. Oral Surg Oral Med Oral Pathol Oral Radiol. 2021. PMID: 33516643
-
Usefulness of contrast-enhanced CT in the evaluation of depth of invasion in oral tongue squamous cell carcinoma: comparison with MRI.Oral Radiol. 2021 Jan;37(1):86-94. doi: 10.1007/s11282-020-00429-y. Epub 2020 Feb 21. Oral Radiol. 2021. PMID: 32086730
-
Magnetic resonance imaging of thymic epithelial tumors.Crit Rev Diagn Imaging. 1996 Aug;37(3):191-259. Crit Rev Diagn Imaging. 1996. PMID: 8872410 Review.
-
Accuracy of Magnetic Resonance Imaging in Detecting Tumor Depth of Invasion in Squamous Cell Carcinoma of the Tongue: A Systematic Review.J Maxillofac Oral Surg. 2023 Sep;22(3):720-727. doi: 10.1007/s12663-023-01886-8. Epub 2023 Apr 25. J Maxillofac Oral Surg. 2023. PMID: 37534361 Free PMC article. Review.
Cited by
-
A nomogram for predicting overall survival of patients with squamous cell carcinoma of the floor of the mouth: a population-based study.Eur Arch Otorhinolaryngol. 2023 Aug;280(8):3867-3875. doi: 10.1007/s00405-023-07971-5. Epub 2023 Apr 18. Eur Arch Otorhinolaryngol. 2023. PMID: 37071145
-
Current State of Artificial Intelligence in Clinical Applications for Head and Neck MR Imaging.Magn Reson Med Sci. 2023 Oct 1;22(4):401-414. doi: 10.2463/mrms.rev.2023-0047. Epub 2023 Aug 1. Magn Reson Med Sci. 2023. PMID: 37532584 Free PMC article. Review.
-
Accuracy of MRI, CT, and Ultrasound imaging on thickness and depth of oral primary carcinomas invasion: a systematic review.Dentomaxillofac Radiol. 2022 Jul 1;51(5):20210291. doi: 10.1259/dmfr.20210291. Epub 2022 Mar 8. Dentomaxillofac Radiol. 2022. PMID: 35230866 Free PMC article.
-
Revolutionizing radiation therapy: the role of AI in clinical practice.J Radiat Res. 2024 Jan 19;65(1):1-9. doi: 10.1093/jrr/rrad090. J Radiat Res. 2024. PMID: 37996085 Free PMC article. Review.
-
Accuracy of magnetic resonance imaging in the assessment of depth of invasion in tongue carcinoma: A systematic review and meta-analysis.Natl J Maxillofac Surg. 2023 Sep-Dec;14(3):341-353. doi: 10.4103/njms.njms_174_22. Epub 2023 Nov 10. Natl J Maxillofac Surg. 2023. PMID: 38273911 Free PMC article. Review.
References
-
- Japan society for head and neck cancer, Cancer registry committee. Report of head and neck cancer registry of Japan clinical statistics of registered patients. 2016. http://www.jshnc.umin.ne.jp/pdf/2016syourei_houkok. Accessed 28 Oct 2020.
-
- Ridge JA, Lydiatta WM, Patel SG, Glastonbury CM, Brandwein-Gensler M, Ghossein RA, et al. et al. Lip and oral cavity. In: Amin MB, Edge S, Greene F, Byrd DR, Brookland RK, Washington MK, et al.et al., editors. AJCC cancer staging manual. 8. New York: Springer; 2017. pp. 79–94.
-
- Baba A, Okuyama Y, Yamauchi H, Ikeda K, Ogino N, Kozakai A, et al. Magnetic resonance imaging findings of styloglossus and hyoglossus muscle invasion: relationship to depth of invasion and clinical significance as a predictor of advisability of elective neck dissection in node negative oral tongue cancer. Eur J Radiol. 2019;118:19–24. doi: 10.1016/j.ejrad.2019.06.023. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
